

Translate this page into:
Usefulness of WBC Count to Mean Platelet Volume Ratio in Predicting Short-Term (30 Days) Major Adverse Cardiac Events in Patients Presenting with Acute Coronary Syndrome and its Comparison in Males and Females
Dr. Sheshidhar Madaka, MD, DM Resident Department of Cardiology NIMS Hyderabad India sheshidharmadaka@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background: Among cardiovascular illnesses, acute coronary syndrome (ACS) events are associated with higher mortality and morbidity. The mechanism of inflammation involved in the ACS includes atherosclerotic plaque development, followed by development of plaque rupture and thrombosis. The present study is to determine whether white blood cell count to mean platelet volume ratio (WMR) can predict short-term (30 days) major adverse cardiac events (MACE) in ACS patients, and also compare WMR and MACE in males and females.
Aim: To detect usefulness of white blood cell (WBC) count to WMR in predicting short term (30 days) MACE in patients presenting with ACS and compare values and MACE events in males and females.
Material and Methods: The present study was conducted in a tertiary-care hospital from September 2020 to December 2020. A total of 60 patients, who presented with ACS and were undergoing percutaneous coronary intervention (PCI), fulfilled the selection criterion; hence, a total of 60 patients were selected for the study after taking informed consent. The clearance from the Institutional Ethical committee (IEC) was obtained prior to the initiation of the study. All the necessary investigations were done in patients who fulfilled the inclusion criteria. The results of the study were systematically selected and analysis done statistically. The study included all patients with clinical suspicion of ACS for more than 18 years and excluded non-ACS patients, patients with malignancy history, inflammatory diseases, autoimmune disorders, infections, and those who are immunosuppressed.
Results: In the present study, receiver operating characteristic (ROC) curve showed cutoff value of WMR as 1059 with area under curve (AUC) of 0.6 (95% CI 0.4–0.9). MACE occurred in 12 patients and mortality occurred in 6 patients. Among MACE, recurrent myocardial infarction (REMI) occurred in 7 (35%) cases, arrhythmias occurred in 5 (25%), and cardiogenic shock occurred in 8 (40%) cases.
WMR with a cutoff value of 1059 was significant and highly accurate in predicting MACE, with sensitivity of 91.6%, specificity of 87.5%, PPV of 64.7%, NPV of 97.6%, and diagnostic accuracy of 88.3%. Compared to males, females have less sensitivity to, high specificity to, and high diagnostic accuracy of WMR ratio in predicting MACE. MACE did not show any gender predilection.
Conclusion: In patients, who presented with ACS, high WMR values were associated with worse short-term outcomes and independently predicted short-term MACE. Compared to males, females have less sensitivity to, high specificity to, and high diagnostic accuracy of WMR ratio in predicting MACE.
Keywords
White blood cell (WBC) to mean platelet volume (MPV) ratio (WMR)
major adverse cardiac events (MACE)
acute coronary syndrome (ACS)
males and females


Introduction
Among cardiovascular illnesses, acute coronary syndrome (ACS) events are associated with higher mortality and morbidity.1 Majority of the cardiovascular disease risk burden will be taken by the Indian subcontinent in the future.2 The mechanism of inflammation involved in ACS includes atherosclerotic plaque development, followed by development of plaque rupture and thrombosis.3
ACS events are not only due to the stenosis of coronary arterial system but also due to other pathophysiological mechanisms involved in the development of acute coronary events. In the development of acute coronary events, leukocytes play an important role through the processes of inflammation.4 Macrophages and T-cells, which are located in the atherosclerotic plaque core, get activated when endothelium is injured, and there is release of cytokines and procoagulants by these cells, which promote the thrombus formation. These mechanisms increase the risk of thrombogenicity and the development of ACS.5
Increased leukocyte (white blood cell [WBC]) count is helpful in predicting clinical outcome in patients with ACS.6 Mean platelet volume (MPV) is a marker of platelet activation is an inflammatory marker, which can be useful in assessing prognosis in patients with ACS.7 As a combination of both these markers (WBC and MPV), WBC count to MPV ratio (WMR) has been recently found as a novel noninvasive marker for predicting long-term outcomes in patients with ACS8. However, the use of this novel marker for assessing prognosis in persons with ACS in Indians is not yet studied. Therefore, in the present study, we are evaluating whether WMR can be useful as a marker of prognosis in Indian persons presenting with ACS.
Aims and Objectives
To detect usefulness of WMR for predicting short-term (30 days) major adverse cardiac events (MACE) in patients presenting with ACS, and also compare values and MACE events in males and females.
Materials and Methods
The present study was conducted in a tertiary care hospital from September 2020 to December 2020. In the present study, the sample size was 60 cases with ACS, which is based on the study by Adam et al, in which the sensitivity of WMR was 69% with mortality rate of 14%, and the minimum sample size required was 25 cases with ACS.9 Inclusion criteria include patients with ACS. ACS patients were identified by using the following criteria: non-ST-segment elevated myocardial infarction (NSTEMI) was diagnosed if persons had increased cardiac enzymes without detectable ST-segment elevation on the electrocardiogram (ECG). STEMI was diagnosed if person complained of typical angina which lasted for more than 20 minutes along with any one of the following features: ST-segment elevation of at least 1 mm in two or more contiguous leads, formation of new Q wave or left bundle branch block (LBBB) formation, and/or two times increase in the cardiac enzymes. Unstable angina (UA) is diagnosed if there is detectable ischemic changes on an ECG without cardiac enzymes elevation.10
A total of 60 patients presenting with ACS, who fulfilled the selection criterion, were studied. The clearance from the Institutional Ethical committee (IEC) was obtained prior to the initiation of the study. Eligible patients for the study were explained about the study and investigations to be conducted, and written informed consent was taken. All the necessary data including age and gender, clinical features, history of diabetes mellitus, hypertension, smoking, alcohol consumption, and tobacco chewing were taken from the eligible patients, and physical examination carried out to assess the vital parameters. Patients were also evaluated for Killip clinical examination classification and New York Heart Association (NYHA) classification.11 12
Laboratory Investigations:
After admission of the patient, blood samples were collected within 30 minutes to measure hematological parameters and conduct biochemical investigations.
An automated hematology analyzer Beckmann Coulter DXH800 was used to measure hematological parameters and liver function tests (LFTs), while serum electrolytes, blood urea nitrogen (BUN) and creatinine (Cr) were measured with Roche Cobas c501 chemistry analyzer. Patients were also evaluated with ischemia markers creatine phosphokinase (CPK), lactate dehydrogenase (LDH), echocardiography, and a 12-lead ECG. Troponin I was measured with Beckmann DXI600.
Electrocardiographic and Enzymatic Analysis:
The eligible patients were subjected to ECG in order to diagnose the type of ACS. A standard 12-lead ECG recorded at a paper speed of 25 mm/sec and at a calibration of 1 mV = 10 mm. STEMI was diagnosed, according to the European Society of Cardiology (ESC) and American College of Cardiology (ACC) criteria, as typical angina lasting longer than 30 minutes, increased creatine kinase-MB (CK-MB) fraction > 200 U/l and/or increased cardiac troponin I more than 2 microgram\L and/ or new ST elevation at the J point in two contiguous leads > 0.2 mV which leads v2-v3 or > 0.1 mV in other leads.13 14
Echocardiography: The patients were evaluated with echocardiography at the time of hospital admission. The left ventricular end-diastolic diameter was measured from the parasternal long axis view, and the left ventricular ejection fraction was measured using the single-plane, Simpson method.
Inclusion Criteria
-
All patients with clinical suspicion of ACS are included.
-
18 to 90 years age people are included.
-
Both gender are included.
Exclusion Criteria
-
Non-ACS patients, patients with malignancy history, inflammatory diseases, autoimmune disorders and infections, and those who are immunosuppressed.
Statistical Analysis
-
Data has been collected, compiled using Microsoft Excel, and statistical analyzed with the help of SSPS v20. Results on continuous variables are presented as mean and standard deviation (SD). Results on categorical variables are presented as percentages. Chi-square test is used to find out the significance of study parameters on a categorical scale between two investigations. Receiver operating characteristic (ROC) curve analysis was conducted to determine prognostic accuracy of WMR in predicting MACE. Continuous variables are analyzed using independent t-tests for normal distribution; otherwise, the Mann–Whitney U-test is employed. All p-values are two-tailed, and p < 0.05 is considered statistically significant.
Results
In this study, a total of 60 patients with ACS were enrolled.
We observed a slightly greater number of males (n = 36, 60%) than females (n = 24, 40%) in the present study, as shown in Table 1.
|
Gender |
Frequency |
Percent |
|---|---|---|
|
Abbreviations: AUC, area under curve; MACE, major adverse cardiac event; WMR, white blood cell count to mean platelet volume ratio. |
||
|
Female |
24 |
40.00% |
|
Male |
36 |
60.00% |
|
Total |
60 |
100.00% |
Comorbidities of patients: Among 60, 36 (60%) had hypertension and 24 did not have hypertension, 21 (35%) were diabetic, 26 (43.3%) were alcoholics, 21(35%) were smokers, and 10 (16.67%) had hypothyroid, as shown in Table 2.
|
Comorbidities |
Frequency |
Percent |
|---|---|---|
|
Hypertension |
36 |
60% |
|
Diabetes |
21 |
35% |
|
Alcoholism |
26 |
43.3% |
|
Smoking |
21 |
35% |
|
Hypothyroidism |
10 |
16.6% |
Diagnosis of patients: Out of 60 patients presenting with ACS, 9 had anterior wall myocardial infarction (AWMI), 8 presented with extensive anterior wall myocardial infarction (EAWMI), 4 presented with inferior wall myocardial infarction (IWMI), 1 with IWMI with complete heart block (CHB), 2 had EAWMI, 5 had inferior wall posterior wall myocardial infarction (IWPWMI), 1 had extensive inferior wall posterior wall myocardial infarction (EIWPWMI), 16 had NSTEMI, and 13 presented with UA, as shown in Table 3.
|
Diagnosis |
Males |
Percentage |
Females |
Percentage |
Total |
Percent |
|---|---|---|---|---|---|---|
|
Abbreviations: AWMI, anterior wall myocardial infarction; EAWMI, external anterior wall myocardial infarction; EIWMI, external inferior wall myocardial infarction; EIWPWMI, external inferior wall posterior wall myocardial infarction; IWMI, inferior wall myocardial infarction; IWMI CHB, inferior wall myocardial infarction complete heart block; IWPWMI, inferior wall posterior wall myocardial infarction; non-ST-segment elevation myocardial infarction; UA, unstable angina. |
||||||
|
AWMI |
7 |
11.66% |
2 |
3.33% |
9 |
15.00% |
|
EAWMI |
5 |
8.33% |
3 |
5.00% |
8 |
13.33% |
|
EIWMI |
0 |
0.00% |
2 |
3.33% |
2 |
3.33% |
|
EIWPWMI |
1 |
1.66% |
0 |
0.00% |
1 |
1.67% |
|
IWMI |
2 |
3.33% |
2 |
3.33% |
4 |
6.67% |
|
IWMI CHB |
1 |
1.66% |
0 |
0.00% |
1 |
1.67% |
|
IWPWMI |
3 |
5.00% |
2 |
3.33% |
5 |
8.33% |
|
NSTEMI |
9 |
15% |
7 |
11.66% |
16 |
26.67% |
|
UA |
7 |
11.66% |
6 |
10.00% |
13 |
21.67% |
|
Total |
36 |
60.00% |
24 |
40.00% |
60 |
100.00% |
Out of 60 patients, 24 had single vessel disease (left anterior descending [LAD] 13, left circumflex [LCX] 2, right coronary artery [RCA] 9), 1 had left main, triple vessel disease, 9 had triple vessel disease, 26 had double vessel disease (LAD LCX 14, LAD RCA 6, LCX RCA 6) disease. Out of 60 patients 15 patients underwent PCI to LAD, 10 patients underwent PCI to RCA, 4 underwent PCI to LCX, 8 underwent coronary artery bypass graft (CABG) surgery, and 1 underwent multivessel PCI.
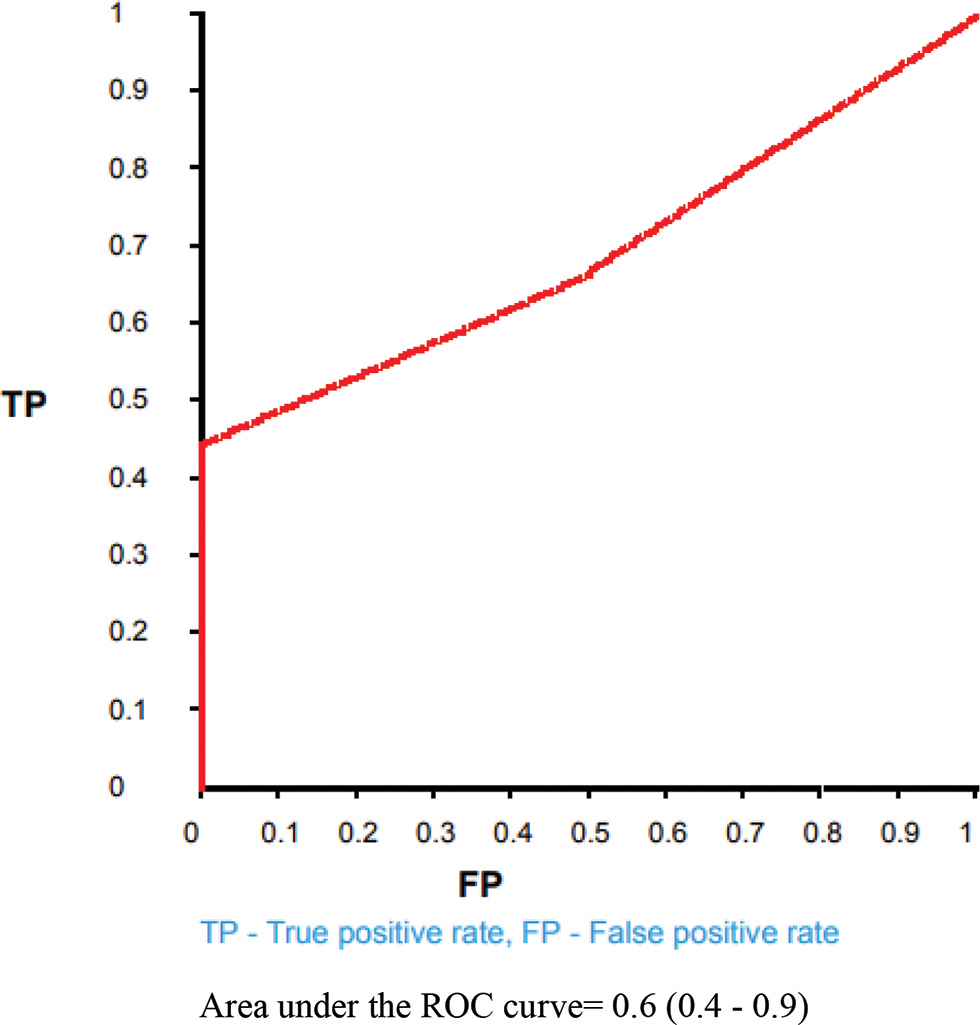
In present study, the ROC curve (as shown in Fig. 1 below) showed cutoff value of WMR as 1059 with area under curve (AUC) of 0.6 (95% CI 0.4–0.9). The area under ROC curve is maximum at 1059 value with better sensitivity.
-
Fig. 1 Receiver operating characteristic (ROC) curve showing area under curve (AUC) for white blood cell count to mean platelet volume ratio (WMR) in predicting major adverse cardiac event (MACE).
Fig. 1 Receiver operating characteristic (ROC) curve showing area under curve (AUC) for white blood cell count to mean platelet volume ratio (WMR) in predicting major adverse cardiac event (MACE).
MACE was noted in 12 patients and mortality was noted in 6 patients. MACE like recurrent myocardial infarction (REMI) occurred in 6 patients with high WMR (> 1059) and in 1 patient with low WMR (< 1059), arrhythmias occurred in 4 patients with high WMR (1059) and in 1 patient with low WMR (1059), and cardiogenic shock occurred in 8 patients with high WMR (1059).
WMR with a cutoff value of 1059 was significant and highly accurate in predicting MACE with sensitivity of 91.6%, specificity of 87.5%, positive predictive value (PPV) of 64.7%, negative predictive value (NPV) of 97.6%, and diagnostic accuracy of 88.3%.
Accuracy Of WMR in Predicting MACE (Overall)
MACE occurred in 12 patients; among them, 11 patients had WMR ratio > 1059 and 1 patient had low WMR ratio < 1059, with sensitivity of 91.6%, specificity of 87.5%, PPV of 64.7%, NPV of 97.6%, and diagnostic accuracy of 88.3% (Table 4).
|
WMR |
MACE |
Total |
p-Value |
|||
|---|---|---|---|---|---|---|
|
Yes |
No |
|||||
|
Abbreviations: CI, confidence interval; MACE, major adverse cardiac event; NPV, negative predictive value; PPV, positive predictive value; WMR, white blood cell count to mean platelet volume ratio. |
||||||
|
>1059 |
11 |
6 |
17 |
0.01 (Significant) |
||
|
</= 1059 |
1 |
42 |
43 |
|||
|
Total |
12 |
48 |
60(100%) |
|||
|
Parameter (patients) |
Estimate |
Lower–upper 95% CIs |
Method |
|||
|
Sensitivity |
91.6% |
(61.5–99.79) |
Wilson score |
|||
|
Specificity |
87.5% |
(74.72–95.27)1 |
Wilson score |
|||
|
PPV |
64.71% |
(45.97–79.80)1 |
Wilson score |
|||
|
NPV |
97.6% |
(86.512– 99.64)1 |
Wilson score |
|||
|
Diagnostic accuracy |
88.3% |
(77.43–95.18)1 |
Wilson score |
|||
|
Likelihood ratio of a positive test |
7.33 |
(3.04–15.8) |
||||
|
Likelihood ratio of a negative test |
0.10 |
(0.012–0.62) |
||||
Comparison of WMR Ratio in Males and Females
In the present study,17 patients had WMR ratio > 1059; among them, 11 were males and 6 were females (Table 5).
|
WMR |
Males |
Percentage |
Females |
Percentage |
Total |
Percent |
|---|---|---|---|---|---|---|
|
Abbreviation: WMR, white blood cell count to mean platelet volume ratio. |
||||||
|
≤ 1059 |
25 |
41.66% |
18 |
30% |
43 |
71.66% |
|
> 1059 |
11 |
18.33% |
6 |
10.00% |
17 |
28.33% |
|
Total |
36 |
60.00% |
24 |
40.00% |
60 |
100.00% |
Accuracy of WMR in Predicting MACE in Females
MACE occurred in 12 patients; among them, 6 patients were females. Among those 6 females, 5 patients had WMR ratio >1059 and 1 patient had low WMR ratio < 1059 with sensitivity of 83.3%, specificity of 94.4%, PPV of 83.33%, NPV of 94.44%, and diagnostic accuracy of 91.67% (Table 6).
|
WMR |
MACE |
Total |
p-Value |
||||
|---|---|---|---|---|---|---|---|
|
Yes |
No |
||||||
|
Abbreviations: CI, confidence interval; MACE, major adverse cardiac event; NPV, negative predictive value; PPV, positive predictive value; WMR, white blood cell count to mean platelet volume ratio. |
|||||||
|
> 1059 |
5 |
1 |
6 |
0.01 (significant) |
|||
|
≤ 1059 |
1 |
17 |
18 |
||||
|
Total |
6 |
18 |
24 |
||||
|
Parameter (patients) |
Estimate |
Lower–upper 95% CIs |
Method |
||||
|
Sensitivity |
83.3% |
(35.88–99.58) |
Wilson score |
||||
|
Specificity |
94.4% |
(72.71–99.861) |
Wilson score |
||||
|
PPV |
83.33% |
(41.86–97.20 1) |
Wilson score |
||||
|
NPV |
94.44% |
(73.89–99.031) |
Wilson score |
||||
|
Diagnostic Accuracy |
91.67% |
(73.00–98.971) |
Wilson score |
||||
|
Likelihood ratio of a positive test |
15 |
(2.162–104.18) |
|||||
|
Likelihood ratio of a negative test |
(0.03–1.06) |
||||||
Comparing WMR and MACE
About 20 MACE events occurred; among them, 18 events occurred in patients with WMR ratio > 1059 and 2 patients had low WMR ratio < 1059, with sensitivity of 90%, specificity of37.5%, PPV of 41.6%, NPV of 88.24%, and diagnostic accuracy of 55% (Table 7).
|
WMR |
MACE |
Total |
p-Value |
||||
|---|---|---|---|---|---|---|---|
|
Yes |
No |
||||||
|
Abbreviations: CI, confidence interval; MACE, major adverse cardiac event; NPV, negative predictive value; PPV, positive predictive value; WMR, white blood cell count to mean platelet volume ratio. |
|||||||
|
> 1059 |
18 (30%) |
25 (41.66%) |
43 (71.66%) |
0.01 (significant) |
|||
|
≤ 1059 |
2 (3.33%) |
15 (25%) |
17 (28.33%) |
||||
|
Total |
20 (33.33%) |
40 (66.66%) |
60 (100%) |
||||
|
Parameter (events) |
Estimate |
Lower–upper 95% CIs |
Method |
||||
|
Sensitivity |
90% |
(69.9–97.211) |
Wilson score |
||||
|
Specificity |
37.5% |
(24.22–52.971) |
Wilson score |
||||
|
PPV |
41.86% |
(28.38–56.671) |
Wilson score |
||||
|
NPV |
88.24% |
(65.66–96.711) |
Wilson score |
||||
|
Diagnostic accuracy |
55% |
(42.49–66.911) |
Wilson score |
||||
|
Likelihood ratio of a positive test |
1.44 |
(1.315–1.576) |
|||||
|
Likelihood ratio of a negative test |
(0.0805–0.8834) |
||||||
|
Diagnostic odds |
5.4 |
(1.096–26.61) |
|||||
Various Types of Major Cardiac Events:
MACE like REMI occurred in 6 patients with high WMR (> 1059) and in 1 patient with low WMR (< 1059), arrhythmias occurred in 4 patients with high WMR (1059) and in 1 patient with low WMR (1059), and cardiogenic shock occurred in 8 patients with high WMR (1059) (Table 8).
|
MACE |
WMR |
Total |
|
|---|---|---|---|
|
≥ 1059 |
< 1059 |
||
|
Abbreviations: MACE, major adverse cardiac event; REMI, recurrent myocardial infarction; WMR, white blood cell count to mean platelet volume ratio. |
|||
|
REMI |
6 (30%) |
1 (5%) |
7 (35%) |
|
Arrythmia |
4 (20%) |
1 (5%) |
5 (25%) |
|
Cardiogenic Shock |
8 (40%) |
0 |
8 (40%) |
|
Total |
18 (90%) |
2 (10%) |
20 (100%) |
Major Adverse Cardiac Events
Overall, 20 MACE occurred in 12 patients. Out of them, 6 were males (10%) and 6 were females (10%). Hence, in the present study, MACE did not show any gender predilection ( and 1 0).
Comparison of Baseline Investigations with WMR (Table 11)
|
Parameter |
WMR (< 1059) (n = 43) |
WMR (> 1059) (n = 17) |
p-Value |
|
|---|---|---|---|---|
|
Abbreviations: ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate aminotransferase; CPK-MB, creatine phosphokinase-MB; HDL, high-density lipoprotein; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; MPV, mean platelet volume; PCV, packed cell volume; PLT, platelet count; TG, triglyceride; VLDL, very low density lipoprotein; WBC, white blood cell; WMR, white blood cell count to mean platelet volume ratio. *Pertains to statistically significant (p ≤ 0.05). |
||||
|
Age |
58 ± 10.399 |
55.2 ± 11.71 |
0.3 |
|
|
Complete blood picture |
Hemoglobin |
11.72 ± 1.27 |
12.511 ± 1.30 |
0.03* |
|
WBC |
9165.116 ± 1557.299 |
14413.529 ± 1795.79 |
< 0.0000001* |
|
|
PCV |
39.72 ± 5.006 |
42.117 ± 5.218 |
0.1 |
|
|
PLT |
1.98 ± 0.407 |
2.5 ± 0.306 |
0.00001* |
|
|
Neutrophils |
7.19 ± 1.55 |
11.37 ± 1.796 |
< 0.0000001* |
|
|
Lymphocytes |
1.62 ± 0.370 |
2.02 ± 0.405 |
0.0005* |
|
|
MPV |
10.82 ± 1.239 |
11.78 ± 1.449 |
0.01* |
|
|
WMR |
840.34 ± 141.83 |
11247 ± 127.65 |
< 0.000001* |
|
|
Cardiac enzymes |
CPK-MB |
259.62 ± 128.55 |
434.823 ± 174.86 |
0.00007* |
|
LDH |
362.72 ± 167.95 |
573.47 ± 206.95 |
0.0001* |
|
|
Liver enzymes |
AST |
63.62 ± 98.86 |
186.529 ± 317.04 |
0.02* |
|
ALT |
56.34 ± 75.146 |
158.647 ± 242.28 |
0.01* |
|
|
ALP |
205.34 ± 68.379 |
201.88 ± 71.37 |
0.8 |
|
|
Bilirubin |
1.011 ± 0.3148 |
1.0176 ± 0.367 |
0.9 |
|
|
Renal parameters |
Blood urea |
23.81 ± 11.11 |
30.117 ± 16.78 |
0.09 |
|
Serum creatinine |
0.934 ± 0.43 |
1.417 ± 1.067 |
0.01* |
|
|
Lipid profile |
Total cholesterol |
170.186 ± 55.23 |
202.70 ± 78.66 |
0.07 |
|
LDL |
120.65 ± 31.65 |
144.23 ± 46.866 |
0.03* |
|
|
HDL |
38.65 ± 3.81 |
36.1176 ± 4.32 |
0.02* |
|
|
TG |
234.093 ± 135.46 |
352.70 ± 158.077 |
0.005* |
|
|
VLDL |
40.27 ± 14.66 |
39.05 ± 13.325 |
0.7 |
|
Comparison of Baseline Investigations with MACE (Table 12)
|
Parameter |
MACE not reported (48) |
MACE reported (12) |
p-value |
|
|---|---|---|---|---|
|
Abbreviations: ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate aminotransferase; CPK-MB, creatine phosphokinase-MB; HDL, high-density lipoprotein; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; MPV, mean platelet volume; PCV, packed cell volume; PLT, platelet count; TG, triglyceride; VLDL, very low density lipoprotein; WBC, white blood cell; WMR, white blood cell count to mean platelet volume ratio. *Pertains to Statistically Significan (p ≤ 0.05). |
||||
|
Age |
58.0625 ± 10.78 |
54.33 ± 10.48 |
0.2 |
|
|
Complete blood picture |
Hemoglobin |
11.745 ± 1.269 |
12.74 ± 1.28 |
0.01* |
|
WBC |
9647.9116 ± 1906.31 |
14669.16 ± 2632.169 |
< 0.0000001* |
|
|
PCV |
40 ± 4.61 |
42 ± 6.87 |
0.2 |
|
|
PLT |
2.066 ± 0.444 |
2.83 ± 0.363 |
0.0000007* |
|
|
Neutrophils |
7.56 ± 1.77 |
11.55 ± 2.47 |
< 0.000001* |
|
|
Lymphocytes |
1.63 ± 0.368 |
2.19 ± 0.336 |
0.00001* |
|
|
MPV |
10.922 ± 1.22 |
11.925 ± 1.611 |
0.02* |
|
|
WMR |
889.375 ± 163.96 |
1220.33 ± 270.55 |
0.000001* |
|
|
Cardiac enzymes |
CPK-MB |
267.29 ± 132.70 |
477.166 ± 166.98 |
0.00001* |
|
LDH |
371.04 ± 171.839 |
628 ± 188.171 |
0.00002* |
|
|
Liver enzymes |
AST |
73.75 ± 182.54 |
197.25 ± 211.11 |
0.04* |
|
ALT |
61.39 ± 119.54 |
181.08 ± 212.08 |
0.01* |
|
|
ALP |
197.125 ± 63.44 |
233.33 ± 83.25 |
0.1 |
|
|
Bilirubin |
0.977 ± 0.269 |
1.158 ± 0.48 |
0.08 |
|
|
Renal parameters |
Blood urea |
23.54 ± 10.65 |
38.33 ± 18.64 |
0.0005* |
|
Serum creatinine |
0.929 ± 0.408 |
1.64 ± 1.21 |
0.001* |
|
|
Lipid profile |
Total cholesterol |
163.58 ± 49.83 |
242.666 ± 75.83 |
0.00004* |
|
LDL |
117.166 ± 29.31 |
168 ± 41.34 |
0.000007* |
|
|
HDL |
38.45 ± 3.89 |
35.83 ± 4.38 |
0.04* |
|
|
TGS |
227.208 ± 125.56 |
429.66 ± 137.30 |
0.000007* |
|
|
VLDL |
39.833 ± 14.509 |
40.33 ± 13.47 |
0.9 |
|
Mean Values of Study Population (Table 13)
|
Parameter |
Mean ± SD |
|
|---|---|---|
|
Abbreviations: ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate aminotransferase; CPK-MB, creatine phosphokinase-MB; HDL, high-density lipoprotein; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; MPV, mean platelet volume; PCV, packed cell volume; PLT, platelet count; SD, standard deviation; TG, triglyceride; VLDL, very low density lipoprotein; WBC, white blood cell; WMR, white blood cell count to mean platelet volume ratio. |
||
|
Complete blood picture |
Hemoglobin |
11.945 ± 1.32 |
|
WBC |
10652.166 ± 28779.07 |
|
|
PCV |
40.4 ± 5.139 |
|
|
PLT |
2.13 ± 0.44 |
|
|
Neutrophils |
8.36 ± 2.49 |
|
|
Lymphocytes |
1.73 ± 0.42 |
|
|
MPV |
11.123 ± 1.355 |
|
|
WMR |
955.56 ± 229.97 |
|
|
Cardiac enzymes |
CPK-MB |
309.266 ± 162.46 |
|
LDH |
422.43 ± 202.158 |
|
|
Liver enzymes |
AST |
98.45 ± 193.22 |
|
ALT |
85.33 ± 148.66 |
|
|
ALP |
204.366 ± 68.64 |
|
|
Bilirubin |
1.01 ± 0.32 |
|
|
Renal parameters |
Blood urea |
25.6 ± 13.13 |
|
Serum creatinine |
1.071 ± 0.699 |
|
|
Lipid profile |
Total cholesterol |
179.4 ± 63.78 |
|
LDL |
127.3 ± 37.73 |
|
|
HDL |
37.93 ± 4.09 |
|
|
TGS |
267.7 ± 150.8 |
|
|
VLDL |
39.9 ± 14.19 |
|
Discussion
WMR is a novel noninvasive marker, which is highly accurate in predicting MACE in patients presenting with ACS. Raised WMR with cutoff value of 1059 with AUC of 0.6 (95% CI 0.4–0.9), sensitivity of 91.6%, specificity of 87.5%, PPV of 64.7%, NPV of 97.6%, and diagnostic accuracy of 88.3% (p = 0.01).
MACE occurred in 12 patients; among them, 6 patients were females. Compared to males, females had less sensitivity to, high specificity to, and high diagnostic accuracy of WMR ratio in predicting MACE.
Overall, 20 MACE occurred in 12 patients. Out of them, 6 were males (10%) and 6 were females (10%). Hence, in the present study, MACE did not show any gender predilection.
Out of 60 patients presenting with ACS, 7 patients developed REMI (11.66%). Among them, 3 were males (5%) and 4 were females (6.66%). Compared to males, females had slight increase of incidence of REMI.
Out of 60 patients presenting with ACS, 5 patients developed arrhythmias (8.33%). Among them, 3 were males (5%) and 2 were females (3.3%). Compared to males, females had slight decrease of incidence of arrhythmias.
Out of 60 patients 8 patients developed cardiogenic shock. Among them, 4 were males (6.66%) and 4 were females (6.66%). Compared to males, females had equal incidence of cardiogenic shock.
Out of 60 patients, death occurred in 6 patients in the present study. Among them, 3 were males (5%) and 3 were females (5%). Males and females had similar death rates.
Out of 60 patients 6 patients died, and cause of death was cardiogenic shock in 5 and arrhythmia in 1 patient. Cause of death in males was cardiogenic shock, and in females, cause of death was cardiogenic shock and arrhythmia.
Along with WMR, higher WBC and higher neutrophil count were other predicators of MACE.
WMR is a ratio derived from WBC count to MPV ratio. In the present study, baseline MPV level in patients with MACE was 11.78± 1.449, and in patients without MACE, it was 10.82± 1.239.
In the present study, mean WBC count was found significantly high in patients with MACE (14669.16±2632.169) than those without MACE (9647.9116±1906.31) and the difference was significant (p < 0.0001). An increased WBC count is a prominent indicator of compromised microvascular reperfusion. Barron et al presented that acute MI patients with a leucocyte count in the highest quintile had a higher 30-day mortality rate than patients with a leucocyte count in the lower quintiles.15 In the present study, it was also found that increased WBC count was associated with MACE.
The present study demonstrated that raised WMR, that is with a cutoff value of 1059, holds greater predictive value for short-term MACE in patients presenting with ACS, yielding higher diagnostic accuracy (88.3%), sensitivity (91%), specificity (87.5%) with low PPV (64.7%) and high NPV (97.6%) as well as high positive likelihood ratio (7.33) and lower negative likelihood ratio (0.10) (p = 0.01). Recently, Adam et al reported sensitivity of 68.3% and specificity of 63.7% with slightly higher WMR cutoff values (1068.75, AUC = 0.734 95% CI: 0.656–0.812; p < 0.001), which is very much comparable with the present study.
The present study results show that WMR had a higher sensitivity to predict short-term outcomes; therefore, calculating WMR is not only sensitive but a faster and a more efficient marker.
Overall, the present study demonstrates that raised WMR (≥ 1059) is highly accurate in discriminating poor outcome, that is, MACE within 30 days of patients presenting with ACS.
However, these conclusions require careful interpretation due to potential limitations of this study
Limitations of this Study
The conclusions drawn from the present study were based on a single-centre study comprising a relatively smaller sample size, using a nonrandomized sampling technique. Furthermore, we did not measure other more specific proinflammatory markers, including P-selectin, high-sensitivity C-reactive protein (CRP), interleukins, selectin molecules, adhesion ligands and receptors, and markers of oxidative stress to show any comparison between WMR and such biomarkers. Further studies are required to validate these results and define the exact role of WMR in predicting short-term MACE.
Conclusion
In patients who presented with ACS, high WMR values were associated with worse short-term outcomes and independently predicted short-term MACE. Compared to males, females had less sensitivity, high specificity, and high diagnostic accuracy of WMR ratio in predicting MACE.
|
MACE |
No. of events |
Percent |
|---|---|---|
|
Abbreviation: MACE, major adverse cardiac event. |
||
|
Yes |
20 |
33.33% |
|
No |
40 |
66.66% |
|
Total |
60 |
100.00% |
|
MACE |
Males |
Percentage |
Females |
Percentage |
Total |
Percent |
|---|---|---|---|---|---|---|
|
Abbreviation: MACE, major adverse cardiac event. |
||||||
|
Yes |
6 |
10% |
6 |
10% |
12 |
20.00% |
|
No |
30 |
50.00% |
18 |
30.00% |
48 |
80.00% |
|
Total |
36 |
60.00% |
24 |
40.00% |
60 |
100.00% |
Conflict of Interest
None declared.
References
- Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997;349:1269-1276. (9061)
- [Google Scholar]
- Epidemiology and causation of coronary heart disease and stroke in India. Heart. 2008;94(01):16-26.
- [Google Scholar]
- Mechanisms of acute coronary syndromes and their implications for therapy. N Engl J Med. 2013;368(21):2004-2013.
- [Google Scholar]
- Women’s Health Initiative Research Group. Leukocyte count as a predictor of cardiovascular events and mortality in postmenopausal women: the Women’s Health Initiative Observational Study. Arch Intern Med. 2005;165(05):500-508.
- [Google Scholar]
- Pathophysiology of atherosclerotic plaque development. Cardiovasc Hematol Agents Med Chem. 2015;13(01):10-13.
- [Google Scholar]
- Which white blood cell subtypes predict increased cardiovascular risk? J Am Coll Cardiol. 2005;45(10):1638-1643.
- [Google Scholar]
- White blood cell count to mean platelet volume ratio is a prognostic factor in patients with non-ST elevation acute coronary syndrome with or without metabolic syndrome. Korean Circ J. 2016;46(02):229-238.
- [Google Scholar]
- Prognostic value of blood count parameters in patients with acute coronary syndrome. Indian Heart J. 2018;70(02):233-240.
- [Google Scholar]
- White blood cell count to mean platelet volume ratio as a novel non-invasive marker predicting long-term outcomes in patients with non-ST elevation acute coronary syndrome. Cardiol J. 2015;22(04):437-445.
- [Google Scholar]
- Validation of the Killip-Kimball classification and late mortality after acute myocardial infarction. Arq Bras Cardiol. 2014;103(02):107-117.
- [Google Scholar]
- Limitations of the New York Heart Association functional classification system and self-reported walking distances in chronic heart failure. Heart. 2007;93(04):476-482.
- [Google Scholar]
- 2015. Harrison's Principles of Internal Medicine, New York, NY: McGraw-Hill Companies
- The association between white blood cell count and acute myocardial infarction mortality in patients > or =65 years of age: findings from the cooperative cardiovascular project. J Am Coll Cardiol. 2001;38(06):1654-1661.
- [Google Scholar]




