

Translate this page into:
A Rare Cause of Right Heart Failure
*Corresponding author: Dr. Rajendra Betham, Department of Cardiology, Guntur Medical College, Guntur, Andhra Pradesh, India. dr.b.rajendra@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ashwini K, Betham R, Nathani S. A Rare Cause of Right Heart Failure. Indian J Cardiovasc Dis Women. 2024;9:185-7. doi: 10.25259/IJCDW_39_2024
Abstract
A 63-year-old female presented with the right heart failure, on evaluation, a two-dimensional echocardiogram showed a huge left atrial mass causing pseudo-obstruction and right ventricular (RV) failure. Following stabilization and prompt tumor excision, the patient’s RV dysfunction improved. Atrial myxomas can manifest as constitutional embolic or obstructive symptoms. Usually, the right-sided myxomas cause RV dysfunction, but, in this case, atrial myxoma caused RV dysfunction with timely intervention the outcome became better.
Keywords
Right heart failure
Left atria
Echocardiogram
Pulmonary arterial hypertension
Pseudo-obstruction

INTRODUCTION
The most frequent benign heart tumor is myxoma. Although myxomas can develop from any chamber, left atrium (LA) is the most prevalent. Myxoma cells may have originated from pluripotent mesenchymal cells in the fossa ovalis, and as a result, they express a range of antigenic markers.[1] The typical age of presentation is between the fifth and sixth decade, with female preponderance. Myxomas can cause constitutional, embolic, or obstructional symptoms.
CASE REPORT
We are presenting a 63-year-old female patient who has been complaining of shortness of breath, that is, New York Heart Association Class III and bilateral pedal edema for the past 10 days. She was evaluated for identical concerns; her hemoglobin was 10 g/dL, and her liver and renal function tests were within normal ranges. Chest radiography demonstrated cardiomegaly and pulmonary edema. Her electrocardiogram (ECG) indicated right-axis deviation and T-wave inversions in the anterior leads. A two-dimensional echocardiography revealed a massive mass that encompassed the whole LA, was freely movable, attached to inter atrial septum, and protruded into the left ventricle, generating obstructive symptoms,[2,3] as well as significant tricuspid regurgitation jet velocity is 3.5 and right ventricle dysfunction in the form of tricuspid annular plane systolic excursion 12 mm with dilated inferior vena cava with normal left ventricular function [Figure 1]. Because the patient is 63 years old, we performed a coronary angiography following stabilization, which revealed normal coronaries. She was subsequently referred to cardiothoracic surgery for excision. They removed that tumor. (Biopsy of tumor in Figure 2). Now that, she has been on follow-up, her right ventricular dysfunction has improved.
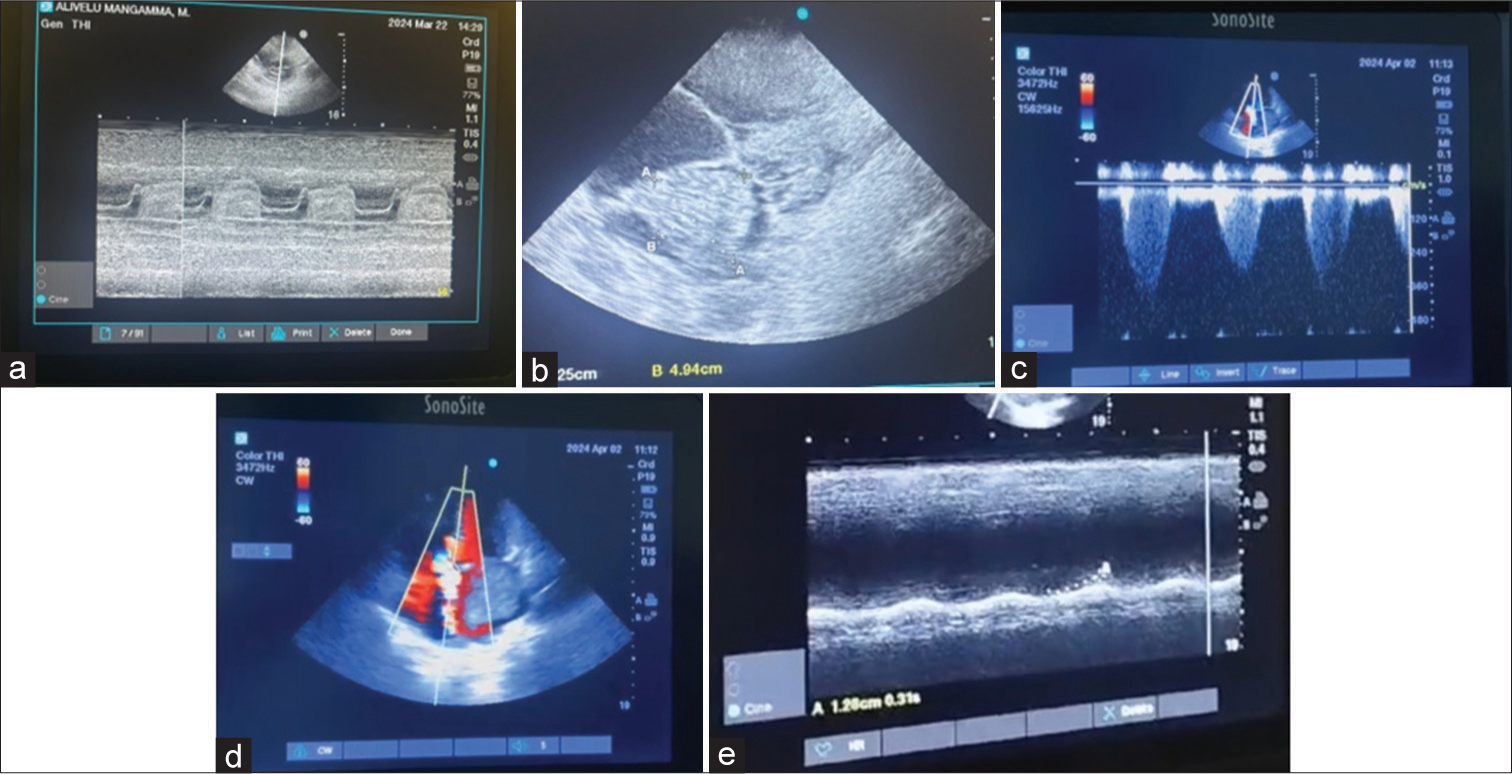
- (a) M mode of two-dimensional echocardiogram, (b) two-dimensional echocardiogram showing left atrium myxoma, (c) four-chamber view showing tricuspid regurgitant jet, (d) color Doppler of apical four-chamber view showing tricuspid regurgitation, and (e) tricuspid annular plane systolic excursion of the patient showing right ventricular dysfunction.
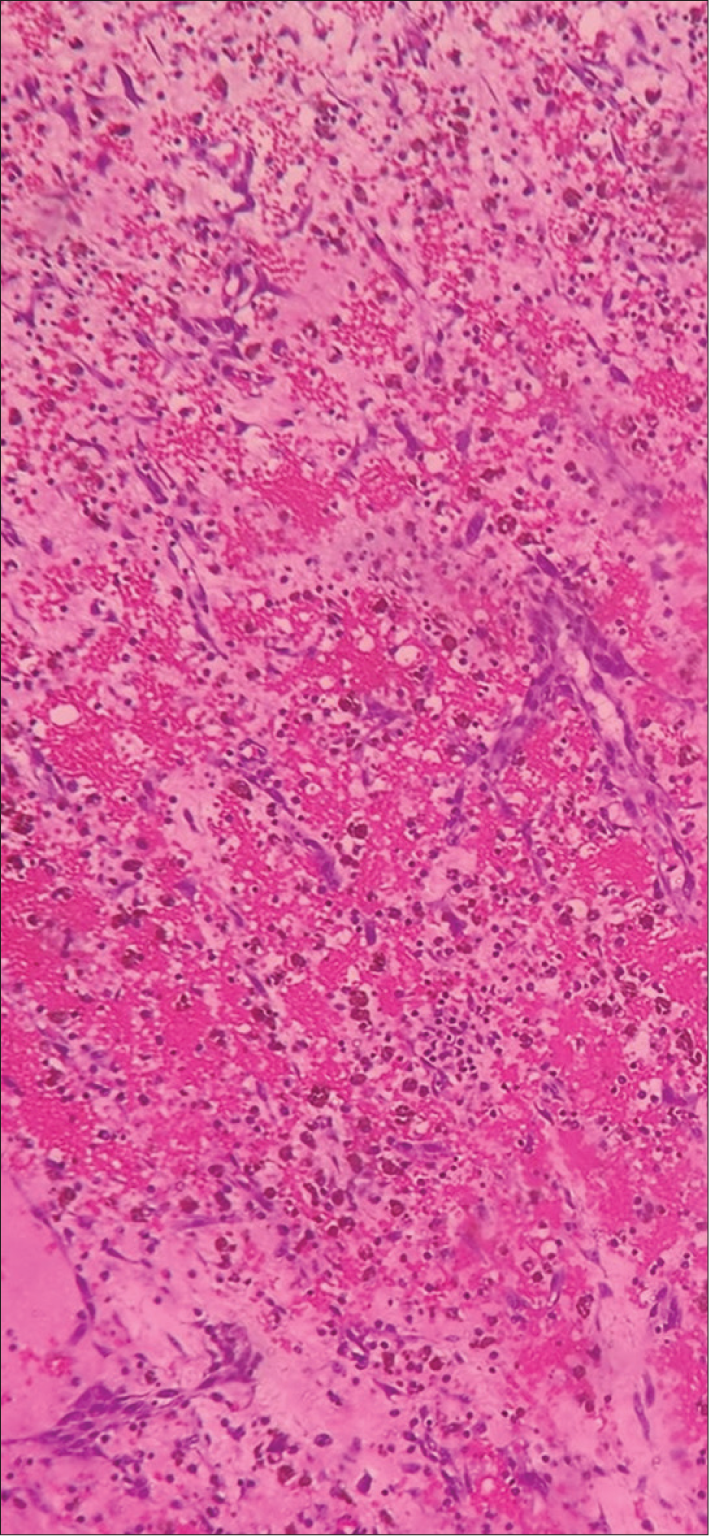
- Hematoxylin and eosin staining of biopsy of the left atrium myxoma.
DISCUSSION
Cardiac myxomas are the most frequent benign heart tumors that can be functionally malignant by obstruction and embolism. They can be sporadic or familial, with the former being the most prevalent appearance.[3] Sporadic atrial myxomas normally develop from the interatrial septum alone. Familial originates from atypical places, and many are rarely found on heart valves linked with the carney complex, which is autosomal dominant due to mutations in genes encoding the cyclic AMP-dependent protein kinase type 1 alpha regulatory subunit.[4] Myxomas are prone to fragmentation[5] and embolism.[6]
Despite the non-specificity of ECG results, echocardiography is frequently necessary for diagnosis.[7] While computed tomography chest imaging can distinguish between a tumor and a thrombus, magnetic resonance imaging helps determine the size and location of tumors.[8] Myxomas frequently necessitate immediate surgery.
CONCLUSION
Myxomas might present with obstructive symptoms as their earliest presentation. The left-sided myxomas can cause right heart failure by generating a pseudo-stenotic lesion.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Cardiac Myxoma: Review and Update of Contemporary Immunohistochemical Markers and Molecular Pathology. Adv Anat Pathol. 2020;27:380-4.
- [CrossRef] [PubMed] [Google Scholar]
- Mitral Pseudostenosis Due to a Large Left Atrial Myxoma. J Geriatr Cardiol. 2018;15:244-5.
- [Google Scholar]
- Giant Left Atrial Myxoma that Caused Mitral Valve Obstruction and Pulmonary Hypertension. Int J Cardiol. 2015;199:38-9.
- [CrossRef] [PubMed] [Google Scholar]
- Benign Cardiac Tumors and Tumorlike Conditions. Ann Diagn Pathol. 2010;14:215-30.
- [CrossRef] [PubMed] [Google Scholar]
- Cerebral Embolism from Atrial Myxoma in Pediatric Patients. Pediatrics. 2003;112:e162-7.
- [CrossRef] [PubMed] [Google Scholar]
- Noninvasive Diagnosis of Bilocular Left Atrial and Right Ventricular Myxoma of the Heart. Z Kardiol. 1988;77:251-5.
- [Google Scholar]
- Incidental Finding of a Left Atrial Myxoma While Characterising an Autoimmune Disease. J Crit Care Med (Targu Mures). 2018;4:64-7.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiac Tumors: Diagnosis, Prognosis, and Treatment. Curr Cardiol Rep. 2020;22:169.
- [CrossRef] [PubMed] [Google Scholar]




