

Translate this page into:
The Uncrossable STEMI – Calcific Eruptive Nodule in Elder ly Women

*Corresponding author: Bharath Raj Kidambi, Department of Cardiology, Kauvery Hospital, Chennai, Tamil Nadu, India. drbkid@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Roy S, Kumar P, Kidambi B, Srikumar S, Veeraraghavan S. The Uncrossable STEMI – Calcific Eruptive Nodule in Elderly Women. Indian J Cardiovasc Dis Women. 2024;9:40-2. doi: 10.25259/IJCDW_62_2023
A 78-year-old lady presented with an inferior wall Myocardial infarction (MI) and was taken up for primary percutaneous coronary intervention (PCI). There was a tight lesion in the proximal Right coronary artery (RCA) [Figure 1a and Video 1], with significant calcified lesions in Left anterior descending artery (LAD) and non-dominant Left circumflex artery (LCX). RCA was engaged with 6 Fr 3.5 Judkins right guiding catheter, and the tight lesion was crossed with 0.014” Run-through wire. Several attempts to cross the lesion failed despite using progressively smaller balloons (1.25 × 10 mm Ryurei, Terumo; 1 × 6 mm Ikazuchi zero, Kaneka; 0.85 × 6 mm Nic Nano, SIS medical), fine cross microcatheter, buddy wire technique, and even with guideliner support [Figure 1b and c]. After a quick heart team discussion with the patient and relatives, it was decided to go with a bail-out calcium debulking strategy. The guide was upsized and the lesion was crossed directly using Rota floppy (Boston Scientific) wire [Figure 1d]. The tight segment was successfully burred using a 1.5 mm rota burr at 150,000 rpm for 15–20 s [Figure 1e]. The patient developed bradycardia and a slow flow phenomenon which was successfully managed. The lesion was predilated with a 2.75 × 9 mm NC Sprinter balloon (Medtronic) which showed dog boning [Figure 1f]. Intravascular ultrasound (IVUS) run demonstrated a diffuse lesion with nearly 360° arc calcium with some breaks after rotablation [Figure 1g and h]. Further, debulking was carried out using 3 × 12 mm intravascular lithotripsy (IVL) (shockwave medical) to avoid slow flow-related complications with burr escalation [Figure 1i]. Consecutive stenting to RCA was done using 3 × 28 mm, 3.5 × 23 mm drug eluting stent (DES) [Figure 1j] and optimized by post-dilating it using a 3.5 × 8 mm Non compliant (NC) balloon. A final IVUS run demonstrated a good stent expansion with an minimal stent area (MSA) of 6.94 mm2 and a good end result [Figure 1k and l and Video 2].
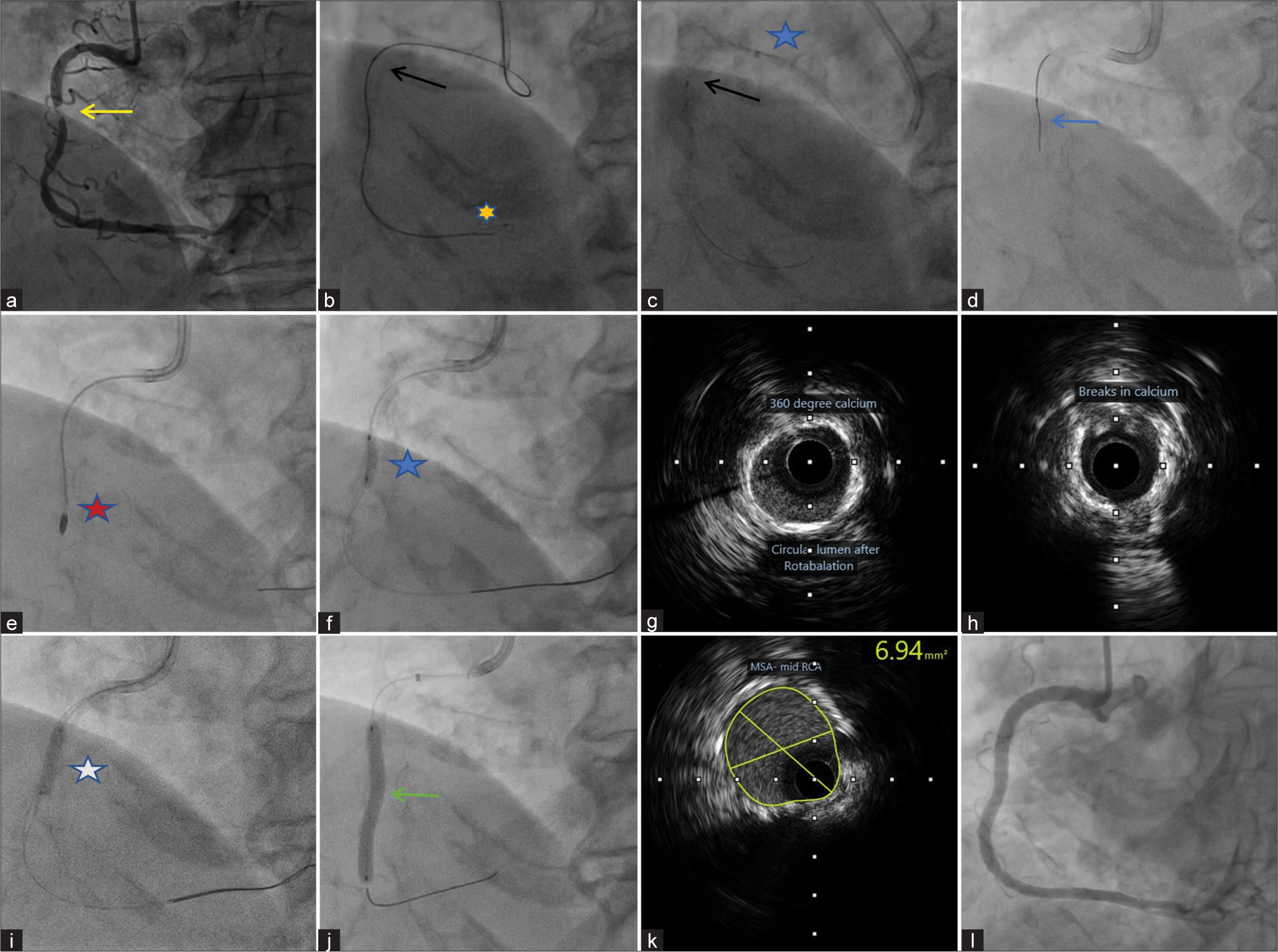
- (a) Coronary angiography left anterior oblique projection (LAO) 30, showing tight lesion in proximal right coronary artery (RCA) (yellow arrow), (b) Fluoroscopic image showing difficulty in crossing the lesion using low profile balloon (black arrow), even with a buddy wire (yellow star), (c) Fluoroscopic image showing difficulty in crossing the lesion using low profile balloon (black arrow) even with guideliner support (blue star), (d) lesion crossed directly using rota floppy wire (blue arrow), (e) rotablation with 1.5 mm red star- rota burr, (f) pre-dilation with 2.75 × 9 mm blue star- dog boning effect while balloon inflation, (g and h) intravascular ultrasound (IVUS) image showing nearly 360° calcium and some breaks after rotablation (i) 3 × 12 mm white star- lithotripsy balloon, (j) stenting with 3 × 28 mm and 3.5 × 23 mm drug eluting stent, with uniform stent expansion (green arrow), (k) post-stent IVUS image yellow circled area- is minimal Stent area (MSA) of 6.94 mm 2, and (l) final angiogram with good end result.
Video 1:
Video 1:Diagnostic angiography and challenges faced in primary percutaneous coronary intervention (PCI) of culprits vessels.Video 2:
Video 2:Successful use of rotablation and lithotripsy as bailout strategy in acute stemi with good end result.An eruptive calcific nodule is an infrequent cause of coronary thrombosis with higher prevalence in the elderly diabetic population. Calcific nodules may limit device cross-ability, leading to stent under-expansion, stent malapposition, and strut damage. High-grade stenotic lesions with complex plaque architecture having both superficial and deep calcium as in our case may need more than one debulking strategy. Utilization of rotablation alone is sometimes burdened with worse outcomes in the Acute coronary syndrome (ACS) subset due to the risk of platelet activation, and no-reflow phenomenon. In such cases, IVL after initial rotablation may act synergistically to cause fractures in deep calcium and achieve good luminal gain with minimal complications.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as the patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Video available on:
Financial support and sponsorship
Nil.




