

Translate this page into:
The Masquerading Tachycardia
Dr. V.S. Bharathi Lakshmi, MD, Associate Professor Department of cardiology, Nizam’s Institute of Medical Sciences India bharathivanaparty@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Fascicular ventricular tachycardia (FVT) often masquerades as supraventricular tachycardia. This article discusses an ECG of FVT and its features, which distinguish it from other mimicking tachycardias.
Keywords
Antidromic AVRT
fascicular ventricular tachycardia
SVT with aberrancy

A 70-year-old male, diabetic and afflicted with chronic obstructive pulmonary disease (COPD), presented with a history of shortness of breath and palpitations since 2 hours. There are no such episodes in the past. What does the ECG suggest?
Opinion 1: atrial tachycardia with right bundle branch block (RBBB), deep s in lead 1 s/o COPD.
Opinion 2: atrial tachycardia.
Opinion 3: ventricular tachycardia.
Author’s response to ECG challenge:
Opinion 4: fascicular ventricular tachycardia (FVT).
Author’s response to ECG challenge:
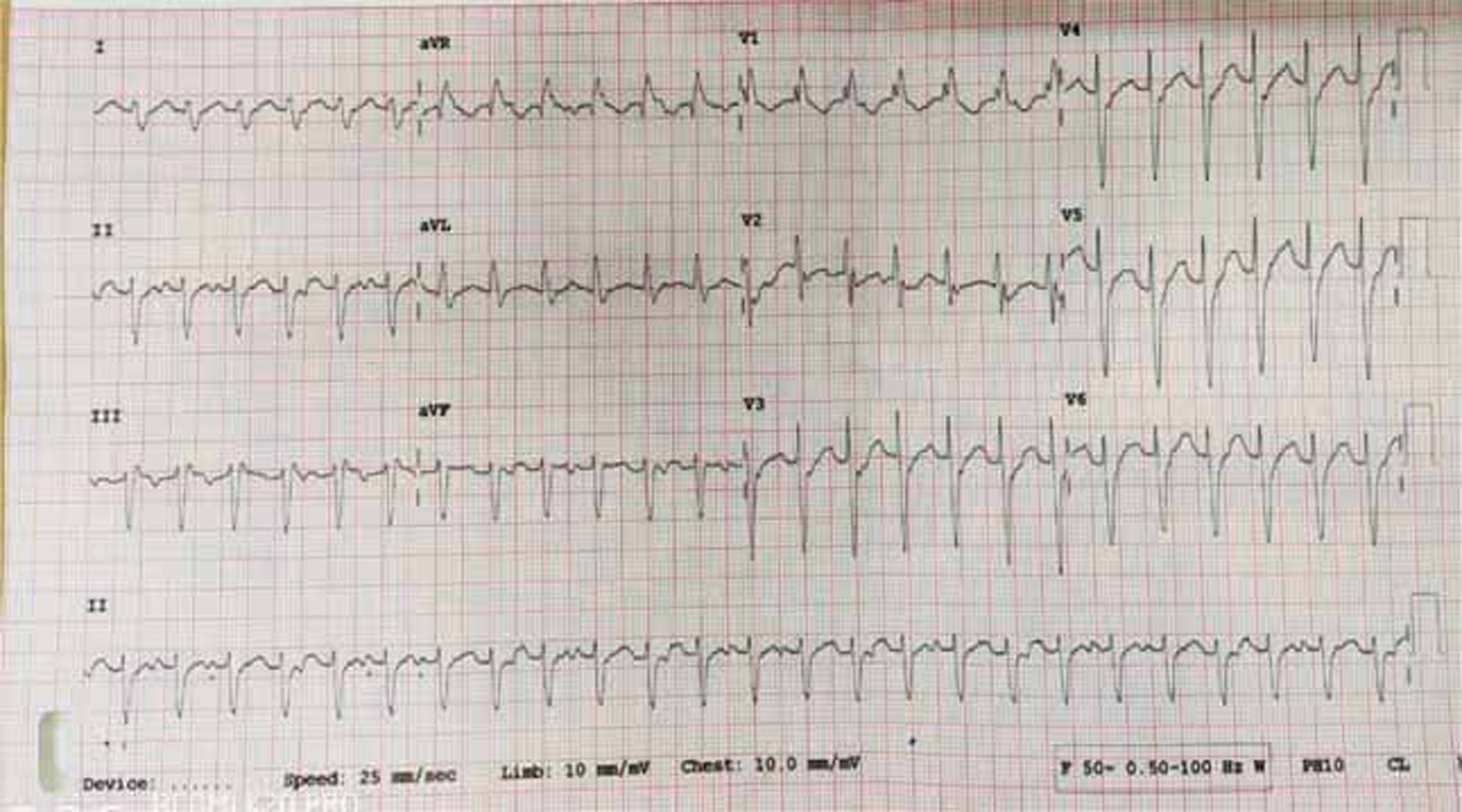
The electrocardiogram in Fig. 1 shows a regular monomorphic wide complex tachycardia (QRS duration of 120 ms). The differential diagnoses are ventricular tachycardia (VT), supraventricular tachycardia (SVT) with aberrancy, and supraventricular tachycardia with antidromic conduction through accessory pathway. The tachycardia has a QRS rate of 150/min with northwest QRS axis, RBBB, and left anterior fascicular block.
-
Fig. 1 Wide complex tachycardia.
Fig. 1 Wide complex tachycardia.
The QRS complexes from V1-V6 are nonconcordant. The R to S duration is 80 ms. The relatively narrow QRS, lack of positive or negative concordance from V1-V6, and the narrow R to S duration may give the impression of SVT with RBBB.1
The northwest axis suggests a VT.2 The rhythm strip in lead 2 (Fig. 2) shows atrioventricular dissociation, which is suggestive of VT. The atrioventricular dissociation has 100% specificity for VT. The RBBB pattern with rS pattern in V6 also suggests VT.3

-
Fig. 2 Rhythm strip showing atrioventricular dissociation.
Fig. 2 Rhythm strip showing atrioventricular dissociation.
The features of antidromic atrioventricular reciprocating tachycardia are inverted P waves with 1:1 conduction, a short PR interval, and a constant RP interval that is usually more than one half the RR interval during tachycardia.4
The above ECG suggests idiopathic left anterior FVT.5 FVT often masquerades as an SVT with RBBB.6 7 FVT is the most common idiopathic VT of the left ventricle. It is also known as Belhassen-type VT or verapamil sensitive tachycardia. It is a reentrant tachycardia, due to an ectopic focus arising in the left ventricle8 9 10. Digoxin toxicity may also cause FVT, but the mechanism involves enhanced automaticity.
Idiopathic fascicular ventricular tachycardia (IFVT) is classified as follows:
-
Left posterior fascicular tachycardia: This is the common type seen in 90 to 95% of the cases. The ectopic focus is near the left posterior fascicle. It occurs with a RBBB and left axis deviation.
-
Left anterior fascicular tachycardia: This type is seen in 5 to 10% of the cases. The ectopic focus arises near the anterior fascicle and occurs with a RBBB and right axis deviation
-
Left upper septal FVT is rare and usually has a RBBB and normal axis. The ectopic focus is near the upper septal region.9
FVT was previously believed to occur in structurally normal heart in young males. It is now known to occur in structurally abnormal heart also.
FVT usually does not respond to adenosine or beta-blockers. It usually responds well to calcium-channel blockers11. Radiofrequency catheter ablation is an alternative therapy for severely symptomatic patients or those intolerant or resistant to antiarrhythmic medication. FVT responds well to radiofrequency ablation.12 13
Conflict of Interest
None declared.
References
- The differential diagnosis of a regular tachycardia with a wide QRS complex on the 12-lead ECG: ventricular tachycardia. supraventricular tachycardia with aberrant conduction and supraventricular tachycardia with anterograde conduction over an accessory pathway. Pacing Clin Electrophysiol. 1994;17:1515-1524.
- [Google Scholar]
- Current algorithms for the diagnosis of wide QRS complex tachycardias. Curr Cardiol Rev. 2014;10(03):262-276.
- [Google Scholar]
- Approach to wide QRS complex tachycardias. In: Issa ZF, Miller JM, Zipes DP. Clinical Arrhythmology and Electrophysiology. 2nd ed. Philadelphia:. Elsevier Saunders 2012:499-511. eds.
- [Google Scholar]
- Differentiation of paroxysmal narrow QRS complex tachycardias using the 12-lead electrocardiogram. J Am Coll Cardiol. 1993;21(01):85-89.
- [Google Scholar]
- Idiopathic paroxysmal ventricular tachycardia with a QRS pattern of right bundle branch block and left axis deviation: a unique clinical entity with specific properties. Am J Cardiol. 1983;52(01):95-100.
- [Google Scholar]
- Idiopathic sustained left ventricular tachycardia: clinical and electrophysiologic characteristics. Circulation. 1988;77(03):560-568.
- [Google Scholar]
- Diagnostic clues from the surface ECG to identify idiopathic (fascicular) ventricular tachycardia: correlation with electrophysiologic findings. J Cardiovasc Electrophysiol. 1996;7(01):2-8.
- [Google Scholar]
- Atrial induction of ventricular tachycardia: reentry versus triggered automaticity. Am J Cardiol. 1979;44(01):1-8.
- [Google Scholar]
- fascicular ventricular arrhythmias: pathophysiologic mechanisms, anatomical constructs, and advances in approaches to management. Circ Arrhythm Electrophysiol. 2017;10:1.
- [Google Scholar]
- Mechanisms of idiopathic left ventricular tachycardia. J Cardiovasc Electrophysiol. 1997;8(05):571-583.
- [Google Scholar]
- Fascicular tachycardia sensitive to calcium antagonists. Eur Heart J. 1984;5(11):896-905.
- [Google Scholar]
- Radiofrequency catheter ablation of idiopathic left ventricular tachycardia guided by a Purkinje potential. Circulation. 1993;88(06):2607-2617.
- [Google Scholar]
- Catheter ablation of idiopathic ventricular tachycardia without the use of fluoroscopy. Int J Cardiol. 2015;190:338-343.
- [Google Scholar]




