

Translate this page into:
Association of Obstructive Sleep Apnea and Coronary Artery Diseases in Women of a Tertiary Care Hospital

*Corresponding author: Mood Narayan, Associate Professor, Department of Pulmonology, Employees State Insurance Corporation Medical College, Hyderabad, Telangana, India. narayana5005@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Malavika TP, Narayan M, Gowda BC. Association of Obstructive Sleep Apnea and Coronary Artery Diseases in Women of a Tertiary Care Hospital. Indian J Cardiovasc Dis Women. 2024;9:201-5. doi: 10.25259/IJCDW_14_2024
Abstract
Introduction:
Obstructive sleep apnea (OSA) exhibits a high prevalence, particularly among individuals possessing established risk factors and concurrent medical conditions. This study aims to elucidate the link between sleep apnea and coronary artery disease (CAD).
Objectives:
The objectives of this study were as follows: To assess the effect of OSA in women with CAD and also to have a comparison with that of men with CAD.
Materials and methods:
It is a case–control study done in 122 patients with OSA. Factors such as age, body mass index, physical activity, frequent junk food intake, and presence of diabetes were assessed.
Results:
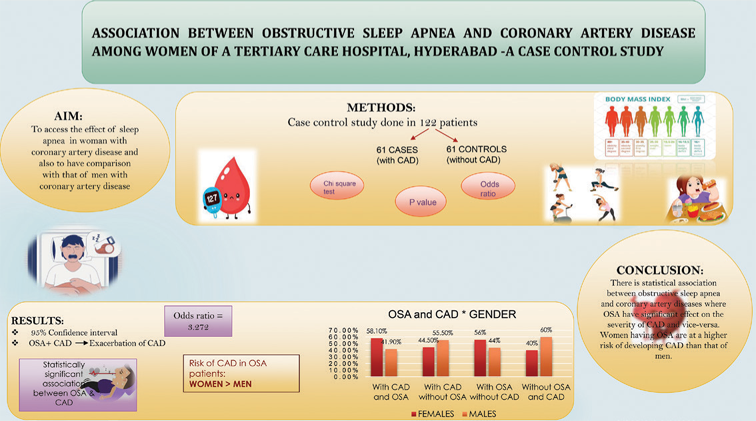
Sixty-one cases having CAD and 61 controls not having CAD were taken. With 95% confidence interval (with an upper level of 6.906 and lower level of 1.550), the odds ratio obtained is 3.272. Hence, there is a statistically significant association between OSA and CAD. At the same time, the study proves that the coexistence of OSA with CAD exacerbates CAD. The study also shows that women with OSA are having increased risk of CAD compared to that of men.
Conclusion:
There is statistical association between OSA and CADs where OSA has a significant effect on the severity of CAD and vice versa. Women having OSA are at a higher risk of developing CAD than that of men.
Keywords
Sleep apnea
Coronary artery disease
Women

ABSTRACT IMAGE
INTRODUCTION
Obstructive sleep apnea (OSA) is a disorder characterized by recurrent instances of the upper airway collapsing and becoming obstructed during sleep, often leading to awakening from sleep, with or without a decrease in oxygen levels. The collapse of the oropharynx at the back of the throat is the primary cause of arousal, oxygen desaturation, or both, ultimately causing disrupted and fragmented sleep.[1] The diagnosis of OSA is confirmed if the number of obstructive events (apneas, hypopneas + respiratory event-related arousals) on polysomnography (PSG) is >5/h in a patient who has any of the following: Unintentional sleep episodes during wakefulness; sleepiness during day time; sleeplessness; fatigue; insomnia; waking up by holding breath, choking; or the bed partner complaining loud snoring, interruptions in breathing, or both during the patient’s sleep.[2]
OSA is classified as:
Mild OSA: Apnea-Hypopnea index (AHI) of 5–15 involuntary sleepiness during activities that require little attention, such as watching TV or reading.
Moderate OSA: AHI of 15–30 involuntary sleepiness during activities that bear some attention, similar as to meetings or donations.
Severe OSA: AHI of more than 30 involuntary sleepiness during conditioning that bear more active attention, similar as talking or driving.[3]
OSA exhibits diverse effects such as pulmonary hypertension, coronary artery disease (CAD), heart failure, amnesia, and diabetes mellitus. The spectrum of effects associated with OSA is daunting. As a result, a large number of complications occurs. Early diagnosis and intervention in case of effects of OSA will be of much help to the patients. Knowledge regarding the spectrum of OSA and CAD in particular in our setting will be valuable to prevent mortality and morbidity. As there are not many studies pertaining to OSA and CAD in women and comparing it to men, this study aims to assess the OSA and CAD in women and its correlation in men.
Aims and objectives
The aims of this study were as follows:
This study was taken with the aim to check the association between obstructive sleep apnea, CAD, and other risk factors.
To assess the effect of OSA in women with CAD.
To have a comparison with that of men with CAD.
MATERIALS AND METHODS
The study was conducted at ESIC Medical College, Hyderabad, in patients attending pulmonology and cardiology outpatients and wards. It is a case–control study done in 122 patients who were classified as cases and controls (61 cases and 61 controls). The study was conducted for a period of 5 months from August 2023 to December 2023.
Patients included in this study are those having OSA and AHI >5, attending cardiology, and general medicine outpatient department above the age of 18 years and given informed consent to participate in study, both groups were included in the study.
Patients with borderline AHI, Chyne stoke breathing, patients received thromboembolitic therapy, and patients who refuses to participate in the study are excluded from the study.
Methodology
A total of 122 patients attending the inpatient and outpatient in the department of pulmonology and cardiology at ESIC Medical College will be studied for a period of 5 months based on their inclusion and exclusion criteria.
Predesigned and pretested questionnaire was used as a data collection tool. This contains sociodemographic details, personal factors, body mass index (BMI) measurements, investigations such as random blood sugar, serum creatine kinase MB (CKMB), serum lactate dehydrogenase (LDH)-1, serum cardiac troponin T and I, arterial blood gas analysis, and liver function test results. Specific symptoms pointing to the diagnosis is also considered.
Polysomnography was conducted to confirm the diagnosis of snoring, tiredness, observed apnea, high blood pressure, body mass index>35, age>50, neck circumference>40, gender male (STOP BANG score), Epworth sleepiness scale (EPSS) score, and berlins questionnaire score which are used for assessing the severity of OSA. In patients of CAD, the disease is confirmed by coronary angiogram using Gensini score.
Statistical analysis was done using SPSS software. Chi-square test is used for categorical type of data for calculation of association between the variables and for calculation of P-value. Odds ratio was used and 95% confidence interval was taken.
RESULTS
This study was conducted in 122 patients and data analysis was done. Among them, 61 were cases and the other 61 belonged to control the group. The mean age of the study population is 52.71 years. Patients included in this study had a mean BMI of 29.01 kg/m2. Equal number of male and female participants was included in this study, which is shown in Figure 1 and Table 1.
- Gender distribution among the study participants.
| Characteristics | Mean | Standard deviation |
|---|---|---|
| Age | 52.71 | 4.172 |
| Height | 154.602 | 4.1627 |
| Weight | 69.34 | 10.404 |
| Neck circumference | 36.417 | 3.7663 |
| Body mass index | 29.0102 | 4.35114 |
From Table 2, major proportion of the study participants belonged to urban population. Occupation of the patients also had a significant impact on our study. It is evident as 52.4% of the patients had a moderate occupation, which accounts to more than half of the study participants.
| Percentage (%) | |
|---|---|
| Residency | |
| Rural | 23.7 |
| Urban | 83.5 |
| Type of occupation | |
| Sedentary | 25.4 |
| Moderate | 52.45 |
| Heavy | 22.13 |
The diagnosis of CAD was confirmed by coronary angiogram using Gensini score. From Figure 2, the mean Gensini score obtained from the patients was 13.7 with a standard deviation of 10.95. The confirmation of OSA was done by polysomnography. The mean AHI obtained from the study was 14.55 with a standard deviation of 11.982.
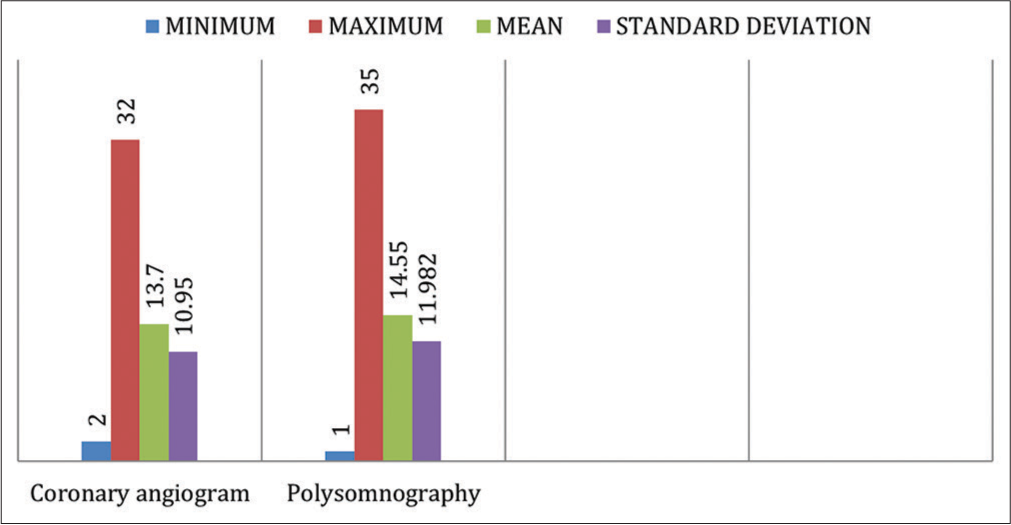
- Diagnosis of CAD and OSA. (CAD: Coronary artery disease, OSA: Obstructive sleep apnea.)
In the 61 cases, who have both OSA and CAD, 58.1% were female compared to 41.9% males. However, in those who were having only CAD, but without OSA, the majority were male with a percentage of 55.5%. Then, in the control group, among people with OSA and without CAD, 56% were female. At the same time, 60% of control groups were not having both OSA and CAD which were found to be males. This indicates that women having OSA are at a higher risk of developing CAD compared to men [Table 3].
| Female | Male | Total | |
|---|---|---|---|
| Cases | |||
| CAD and OSA | 25 | −18 | 43 |
| 58.1% | 41.9% | 100.0% | |
| CAD without OSA | 8 | 10 | 18 |
| 44.5% | 55.5% | 100.0% | |
| Controls | |||
| Without CAD | 14 | 11 | 25 |
| 56.0% | 44.0% | 100.0% | |
| Without OSA and CAD | 14 | 21 | 35 |
| 40.0% | 60% | 100.0% | |
| Total | 61 | 61 | 122 |
CAD: Coronary artery disease, OSA: Obstructive sleep apnea
Pearson Chi-square value obtained in this study was 9.962 with degree of freedom 1 and P = 0.002. This shows that there is a statistically significant association existing between OSA and CAD.
Risk estimate
With 95% confidence interval, the odds ratio obtained was 3.272 with a lower limit of 1.550 and an upper limit of 6.906. This indicates that there is an increased risk of CAD in patients with OSA.
DISCUSSION
OSA seems likely to predispose individuals to the development of CAD, many studies show that there is strong association between OSA and CAD and a few studies demonstrate that there is no association between OSA and CAD.
In our study of 122 study participants, there is a positive association existing between OSA and CAD, which is statistically significant. Minimum age of the patients in this study is 37 and maximum age is 59 with mean age of patient being 52 years. Mean height of the patients is 154 cm, mean weight is 69 kg, mean circumference is 36, and mean BMI is approximately 29 kg/m2. In the study conducted by Wali et al.,[4] the mean age of the patient was 57 years and mean BMI was 30.9 kg/m2 which is similar to the present study.[4] Overweight with short stature and high neck circumference further adds to the factor contributing to the development of CAD. Obesity also leads to poor insulin tolerance, hyperglycemia, and hypoxia making them at high risk for OSA.[5] A study by Kamble and Kanase suggest that obesity is an important risk factor for OSA in obese women with BMI above 30 kg/m2.[6]
In the present study, 50% are male and 50% are female. That means that there is an equal male-to-female ratio. Contrary to the study conducted by Wali et al.,[4] where males are predominant, constituting 72%. This may be due to low sample size in our study. However, from the present study, women with OSA are having increased risk of developing CAD.
The patients belonging to urban areas account for 84% in the present study, and 16% of the patients are from rural backgrounds. Increased urbanization with change in the lifestyle and sedentary life with add on junk and preserved foods contribute to the development of obesity which is a major risk factor for coronary artery Disease. Then, the majority of the patients in this study are home makers followed by business which gives us the clue that sedentary life with increased stress leads to the development of CAD. Furthermore, the majority of the individuals are illiterate.
A study conducted by Loke et al., says that OSA appears to be associated with stroke, but the relationship with ischemic heart disease and cardiovascular deaths was non-significantly associated.[7]
In the present study, 65% of the individuals have shortness of breath, 57% of individuals have excessive day time sleepiness. Cough was seen only in 32% of individuals. About 9% of individuals have decreased sleep during night with night awakenings. Snoring was the major symptom, followed by apnea dizziness and other respiratory complaints. Day time fatigue was one of the major complaints of the patients. The mean blood sugar level was 194 ± 55.45 mg/dL which suggests that the majority of the patients were hyperglycemic. Mean creatine kinase -myocardial band (CKMB) and lactate dehydrogenase (LDH) were 2.4 ± 1.89721 and 212 ± 40.65103, respectively. Mean Troponin I is 0.125 ± 0. 18486 and Troponin T is 0.20 ± 0.12835. This value suggests that hyperglycemia is also associated with OSA. In the study by Wali et al., majority of the patients are diabetic which is similar to the present study.[4] The present study has mean STOP BANG score as 4.26 ± 1.978, EPSS score as 10.53 ± 4.91, and mean AHI 14.55 ± 11.982. In a study conducted by Sorajja et al., mean AHI was 20.17 which is higher than the present study. This could be due to the small sample size of the present study.[8] Spirometry was done in the present study and the majority of the participants showed moderate obstruction followed by mild and severe.
The present study has 62% of the patients with OSA having CAD. In the study by Wali et al.,[4] the prevalence of OSA among the CAD patients was 56.4% which is almost similar to the present study. A similar study from Sweden enrolled 142 men undergoing evaluation of suspected CAD, along with 50 age-matched volunteers; 6% of the control subjects had OSA, compared with 24% of those in the symptomatic group.[9] In a study conducted by Vasheghani-Farahani et al., there is an association of OSA with increased risk of cardiovascular diseases such as CAD, myocardial infarction (MI), and also hypertension.[10]
With a 95% confidence interval (with an upper level of 6.906 and lower level of 1.550), the odds ratio obtained in this study is 3.272. This indicates that there is significant association existing between the two variables in our study, that is, OSA and CAD. In the study conducted by Vasheghani-Farahani et al., they showed that the independent association between OSA and CAD, indeed after adaptation for traditional confounders, suggests that, OSA should be taken into account when considering threat factors for CAD.[10] In contrast, Loomba et al. reported inconsistent findings on the link between OSA and incident or prevalent AF and CAD, with statistically significant results arising mainly from retrospective studies.[11]
In a study by Weinreich et al., ≥50 years OSA is associated with subclinical atherosclerosis in men aged ≤65 years and in women of any age, independent of traditional cardiovascular risk factors was proved.[12] Gami et al.[13] reported that OSA was not independently associated with incident AF in patients above the age of 65 years.[13] In a study by Wang, et al., in hospitalized patients, OSA is associated with increased risk of cardiovascular diseases like CAD particularly among women than men.[14] Confounders such as age, education, alcohol, smoking, obesity, and exercise were reduced and did not affect OSA and CAD. In a study by Macek et al., OSA should be considered an independent predictive factor of a high risk of significant CAD, based on the coronary artery calcium score.[15] This study is similar to the present study.
Limitations of the study
The present study comprised a relatively small number of participants
Being a hospital-based study, there was referral bias with more symptomatic patients likely to be referred to hospital
Another limitation of the present study was the observation of non-significant association between OSA and high-density lipoprotein-cholesterol
Not a multicentric study
Future studies should use a great number of subjects to meet the predicted sample size. There is a need for longitudinal study which would be able to prove whether OSA precedes and causes MI or vice versa
CONCLUSION
Our study demonstrated that many patients with OSA are at the risk of developing CAD. This association could lead to significant repercussions as OSA worsens CAD. Therefore, clinicians should be aware of the coexistence of these two conditions to prevent the development of CAD and decrease the mortality of the patients and to start the treatment at the earliest for better outcome.
Acknowledgment
I thank all the members of PSS and IJCDW society, all patients who have given consent and participated in my study and also, I thank my friend who have helped and encouraged me for doing this research work.
Ethical approval
The research/study approved by the Institutional Review Board at ESIC Medical College, Sanathnagar, Hyderabad, number ESICMC/SNR/IEC-S0289/11-2023, dated 28th November 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Audio summary available at
Financial support and sponsorship
Prajwalika student scholarship.
References
- Obstructive Sleep Apnea Basics. Cleve Clin J Med. 2019;86(9 Suppl 1):2-9.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical Guideline for the Evaluation, Management and Long-term Care of Obstructive Sleep Apnea in Adults. J Clin Sleep Med. 2009;5:263-76.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive Sleep Apnea. J Pharm Bioallied Sci. 2017;9(Suppl 1):S26-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Obstructive Sleep Apnea among Patients with Coronary Artery Disease in Saudi Arabia. J Saudi Heart Assoc. 2015;27:227-33.
- [CrossRef] [PubMed] [Google Scholar]
- How to Define Obesity? Evidence-based Multiple Action Points for Public Awareness, Screening, and Treatment: An ExAsian-Pacific Recommendations. Asia Pac J Clin Nutr. 2008;17:370-4.
- [Google Scholar]
- Association of Obstructive Sleep Apnea with Risk of Serious Cardiovascular Events: A Systematic Review and Meta-analysis. Circ Cardiovasc Qual Outcomes. 2012;5:720-8.
- [CrossRef] [PubMed] [Google Scholar]
- Independent Association between Obstructive Sleep Apnea and Subclinical Coronary Artery Disease. Chest. 2008;133:927-33.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive Sleep Apnoea and Coronary Artery Disease. J Thorac Dis. 2018;10(Suppl 34):S4212-20.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive Sleep Apnea and Severity of Coronary Artery Disease. Caspian J Intern Med. 2018;9:276-82.
- [Google Scholar]
- Association between Sleep Apnea Hypopnea Syndrome and the Risk of Atrial Fibrillation: A Meta-Analysis of Cohort Study. Biomed Res Int. 2018;2018:5215868.
- [CrossRef] [PubMed] [Google Scholar]
- Association of Obstructive Sleep Apnoea with Subclinical Coronary Atherosclerosis. Atherosclerosis. 2013;231:191-7.
- [CrossRef] [PubMed] [Google Scholar]
- The Prevalence of Obstructive Sleep Apnea in Patients with Atrial Fibrillation. Clin Cardiol. 2018;41:601-7.
- [CrossRef] [PubMed] [Google Scholar]
- Association of Obstructive Sleep Apnoea with Cardiovascular Events in Women and Men with Acute Coronary Syndrome. Eur Respir J. 2023;61:2201110.
- [CrossRef] [PubMed] [Google Scholar]
- Obstructive Sleep Apnea as a Predictor of a Higher Risk of Significant Coronary Artery Disease Assessed Non-Invasively Using the Calcium Score. Life. 2023;13:671.
- [CrossRef] [PubMed] [Google Scholar]




