

Translate this page into:
Expert’s Opinion–Challenging ECG

Seema Kale, MD Apollo Clinic, C-70, Rajouri Garden, New Delhi India drseemakale@hotmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Varying kinds of AV blocks can occur in the setting of myocardial ischaemia or due to degeneration of conduction system. Wenckebach AV block can present with typical Wenckebach periodicity or atypical periodicity. A variant of atypical Wenckebach periodicity may present like Mobitz II AV block. This is called Pseudo Mobitz II AV block. As we are aware that Mobitz II AV block is more dangerous and can suddenly convert into complete heart block, it is essential that we should try to differentiate between Mobitz and Pseudo Mobitz II blocks. Infact atypical Wenckebach cycles are quite common at both AV node and his Purkinje system.
Keywords
AV blocks
tachycardia
Wenckebach
Mobitz II
sinus
atypical
pseudo Mobitz II

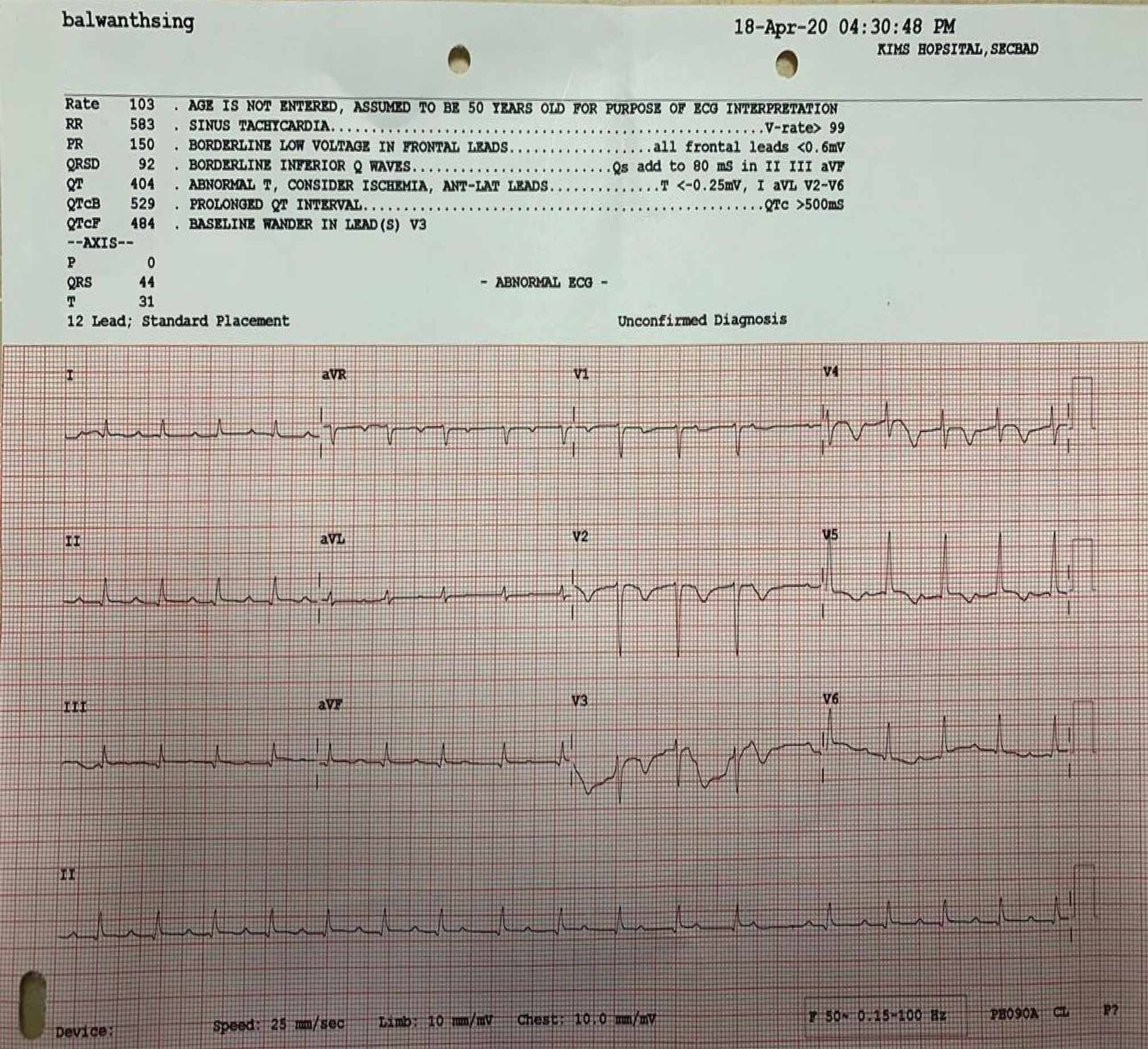
Received ECG (Fig. 1) for the interpretation but no clinical history is available.
-
Fig. 1 Please tell what’s the rhythm.
Fig. 1 Please tell what’s the rhythm.
First Opinion
Narrow complex rhythm, slightly irregular at places, Normal axis, ST-T changes in anterolateral leads suggestive of coronary artery disease (CAD). P wave is not clearly seen, as they are deforming.
T waves, so the T is flat and what we are seeing is P wave. There is 1st degree atrioventricular (AV) block; also, in the middle of strip, Wenckebach block is seen.
Second Opinion
Wenckebach block, PR progressively prolonged and dropped QRS.
Third Opinion
There is prolonged PR interval and 1st degree heart block with old anterior septal myocardial infarction (MI).
Presenter’s Opinion
Sinus tachycardia with first degree AV block. AV Wenckebach starts after 7th complex. With ST-T changes in anterolateral chest leads, s/o CAD. There is low voltage in limb leads (by sensitivity criterion) with poor R wave progression in chest leads, which may be due to obesity.
Response to ECG Challenge: Dr. Somasekhar D, DM
An irregular narrow QRS tachycardia: What is the diagnosis?
ECG is suggestive of arrhythmia in the setting of recent or indeterminate age MI.
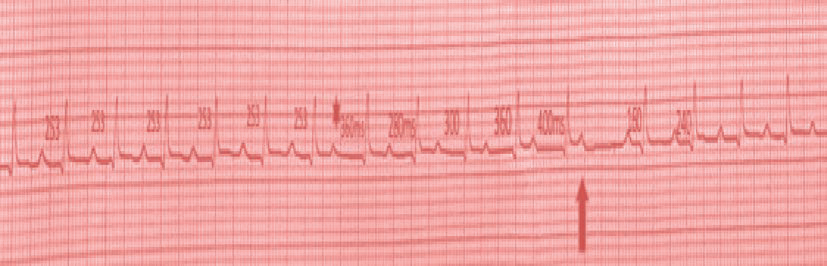
First half of ECG showing sinus tachycardia at heart rate (HR) of 105 beats per minute (BPM) (PP interval of 569 msec) with PR interval of 250 msec and constant PR interval till 7th cycle. There is sudden change in P wave morphology and PP interval (473 msec), which is suggestive of ectopic atrial activity (Fig. 2).
-
Fig. 2 Showing rhythm strip of ECG with fixed PR interval in initial cycles and ectopic P triggering Wenckebach periodicity.
Fig. 2 Showing rhythm strip of ECG with fixed PR interval in initial cycles and ectopic P triggering Wenckebach periodicity.
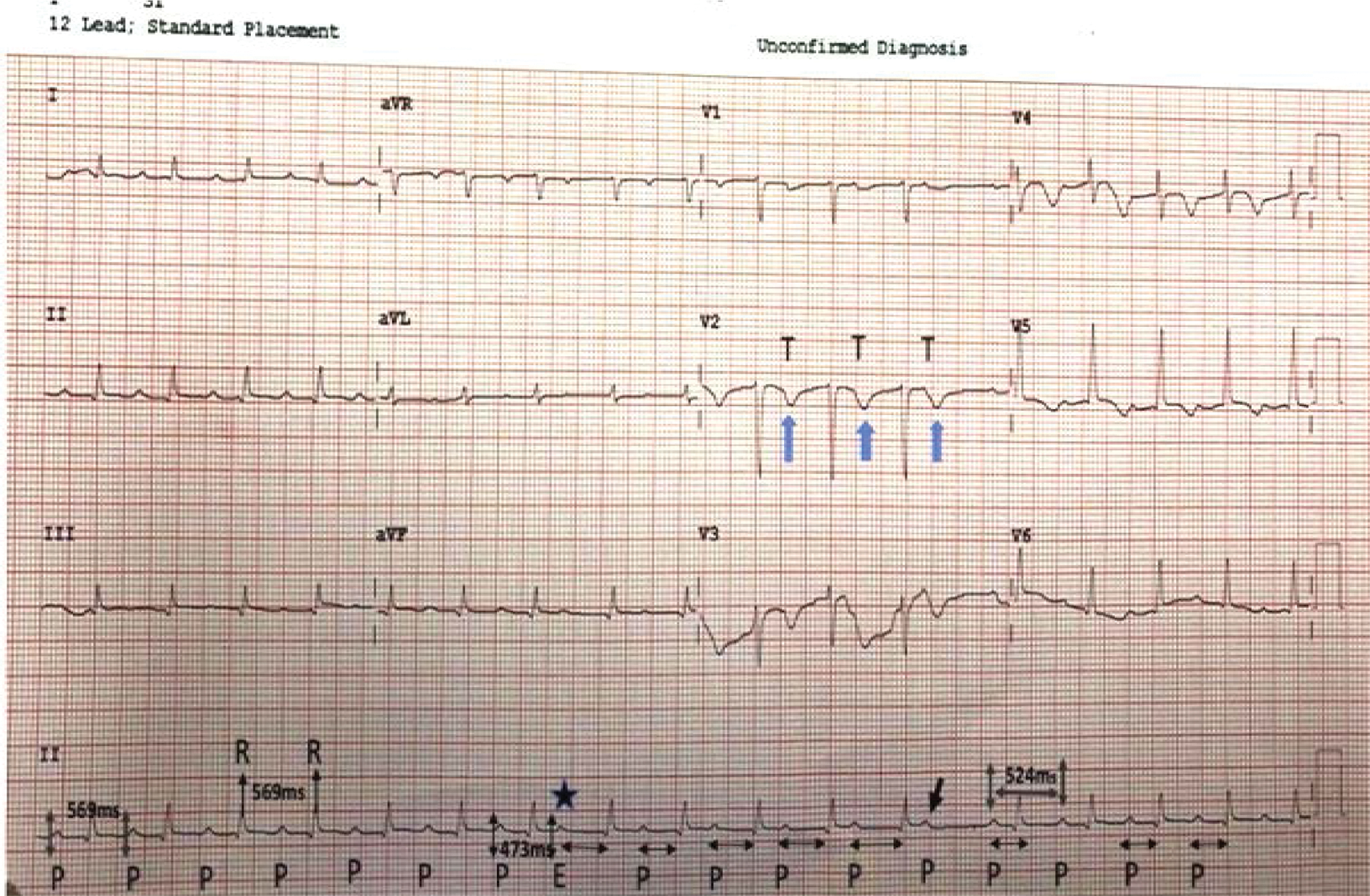
Subsequent P waves, although, resume same morphology as initially with cycle length of 560 msec; there is progressive prolongation of PR interval and block of 5th cycle with a pause. PR interval after pause is 160 msec and PP interval is 540 msec. There is prolongation of PR interval to 230 msec by 2nd complex with continuation of same interval, which is suggestive of atypical Wenckebach periodicity. This atypical Wenckebach periodicity with mild and constant PR prolongation (253 msec) in initial cycles and last three cycles (240 msec) is likely due to associated infra-Hisian disease. Wenckebach periodicity is unmasked by ectopic P wave by altering refractory period and slow conduction across AV node, leading to block. Multiple level conduction abnormalities1 due to ischemia can explain atypical Wenckebach block in this ECG. Low-voltage complexes in limb leads with poor R wave progression in precordial leads and T inversions in precordial leads suggest recent infarct in anterior wall and ischemic etiology for conduction abnormality (Figs. 3 4).
-
Fig. 3 Sinus tachycardia with mild prolonged PR interval, 253 msec, up to 7th cycle associated with PP and RR interval of 569 msec. P wave marked labeled E as premature atrial ectopic with coupling interval of 473 msec conducted with prolonged PR interval, which lead to progressive prolongation of PR even by subsequent normal P waves at PP interval of 560 msec. Blocked P wave is annotated by bold arrow. Immediate P wave after pause is conducted normally (160 msec). Last three P waves conduced with mild PR prolongation of 240 msec, as seen in the initial part of ECG. Precordial leads showing small R waves with T inversions and mild ST coving with T inversion in V4 to V6 second anterolateral infarction.
Fig. 3 Sinus tachycardia with mild prolonged PR interval, 253 msec, up to 7th cycle associated with PP and RR interval of 569 msec. P wave marked labeled E as premature atrial ectopic with coupling interval of 473 msec conducted with prolonged PR interval, which lead to progressive prolongation of PR even by subsequent normal P waves at PP interval of 560 msec. Blocked P wave is annotated by bold arrow. Immediate P wave after pause is conducted normally (160 msec). Last three P waves conduced with mild PR prolongation of 240 msec, as seen in the initial part of ECG. Precordial leads showing small R waves with T inversions and mild ST coving with T inversion in V4 to V6 second anterolateral infarction.
-
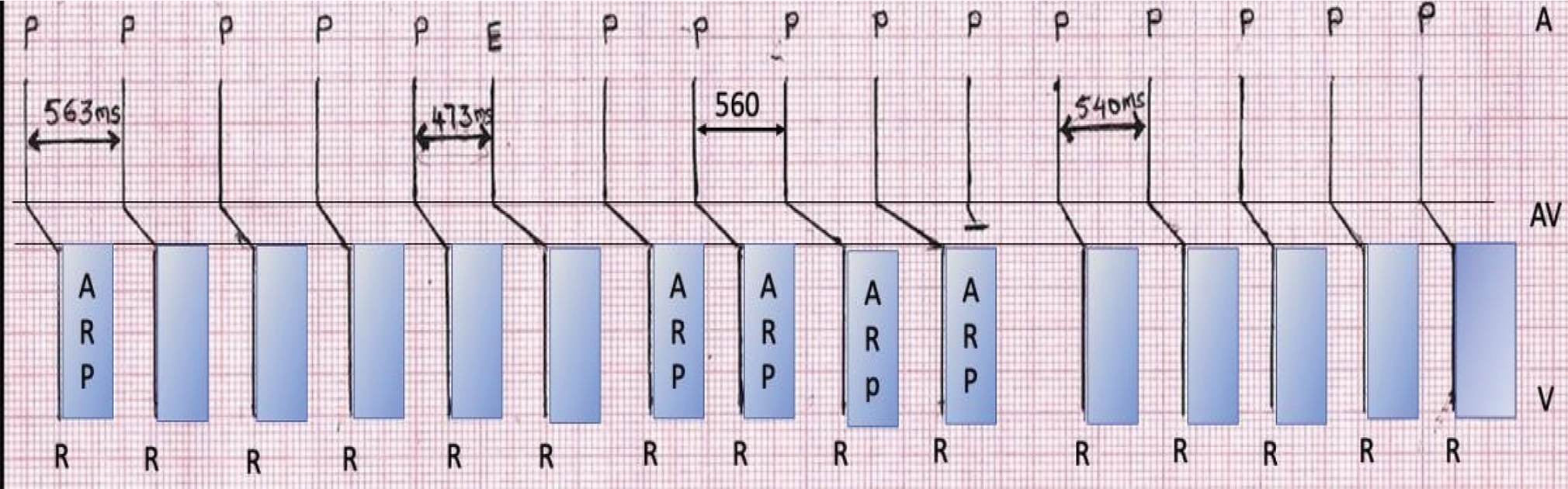
Fig. 4 Ladder diagram showing conduction from atrium to ventricle with conduction delay at AV node level. Ectopic P wave (E) conducted slowly through AV node, causing impulse encroaching on relative refractory period of AV node. Subsequent P waves also impinged on the relative refractory period, with progressive PR prolongation culminating in AV block, when atrial impulse approaches AV node in absolute refractory period of AV node.
Fig. 4 Ladder diagram showing conduction from atrium to ventricle with conduction delay at AV node level. Ectopic P wave (E) conducted slowly through AV node, causing impulse encroaching on relative refractory period of AV node. Subsequent P waves also impinged on the relative refractory period, with progressive PR prolongation culminating in AV block, when atrial impulse approaches AV node in absolute refractory period of AV node.
Typical Wenckebach: Considered to be present when:2
-
The first PR interval of a cycle is the shortest.
-
Progressive lengthening of the PR interval, with the increment between the first and second conducted beats being the largest.
-
Progressive decrease in the RR (VV) intervals.
-
Pause produced by the nonconducted P wave equals the difference between the last PR (before the pause) and the first PR (after the pause) subtracted from twice the PP interval.
Atypical Wenckebach pattern: If failed to meet one or more criteria for typical Wenckebach periodicity.
A pseudo Mobitz II AV block: Defined as long Wenckebach cycle in which, at least, the last three beats of the cycle show relatively constant PR interval (variation of no more than 0.02 second in surface ECG and no more than 10 msec in His bundle electrogram) and in which the PR interval following the blocked beat is shorter than the PR interval before the blocked beat by 0.04 second or more.
Mobitz type I AV block and Type II AV block occurs due to complex interplay of various factors at multiple levels. Careful analysis of ECG is important for management and prognosis. In Mobitz type 2 AV block, we need to be more vigilant, as its response to atropine is less if it progresses to complete heart block (CHB). Mobitz type I AV block in setting of ischemia can also occur due to His Purkinje disease, especially in anterior wall MI and needs careful monitoring.
How to Differentiate between Pseudo Mobitz II and Mobitz II AV Block on Surface ECG?
It is very important that we differentiate between the two, as Mobitz II may suddenly progress to CHB and escape rhythm may not emerge, leading to Stokes–Adams attack and cardiac arrest.
The answer lies in” PR interval” and QRS width.
Pseudo Mobitz II: has relatively constant PR interval in last few beats, but PR interval just before the dropped beat will be longer than PR interval just after the dropped beat by at least one small segment (0.04 s), and QRS is generally narrow.
Mobitz II: PR interval in this is clock regular constant!! And there is sudden drop of beat without any change in PR interval. QRS is generally wide.
Pseudo Mobitz type II and different levels of block
In this, block can occur at AV node and also in His Purkinje system.
Block at AV node:
-
generally associated with acute inferior MI.
-
intraventricular conduction is normal.
-
PR interval in 1st beat of Wenckebach cycle is long, generally around 0.3 second or more.
Block at His Purkinje level:
-
associated with acute anterior MI.
-
associated with right bundle branch block (RBBB) or left. Anterior fascicular block.
-
PR interval of 1st beat in Wenckebach cycle is around 0.26 second or less.
Conflicts of Interest
None declared.
References
- Atypical Wenckebach periodicity simulating Mobitz II AV block. Br Heart J. 1978;40(12):1376-1383.
- [Google Scholar]




